Practical Microbiology: Processing AFB Cultures
AFB = acid fast bacilli
Processing acid fast bacilli cultures takes quite a bit of time. In fact, it usually occupies a third of my 10-hour shift. I often do them along side of fungal cultures (in a different safety hood). It is one of the cultures with the longest turnaround time. The stains, while cannot definitely disprove the presence of AFB, can be useful. Clinicians can use the preliminary results to determine a path of treatments.
Depending on the source of samples, a decontamination process precedes the staining process. This is to prevent other microbes from growing in the AFBs. For samples from sterile sites, the lab does not need to decontaminate, if gram stains show no growth.
The goal of these cultures is to isolate acid fast bacilli. They include tuberculosis, leprosy, and Nocardia. For those who are curious, CDC designates this process under Biosafety Level 3 (BSL-3). That's about as far as I go in terms of training.
The gist of the process goes like this:
- Decontamination
- Inoculate MGIT (mycobacteria growth indicator tubes), LJ slant, and AFB slides
- Staining via auramine-rhodamine (AR) stain
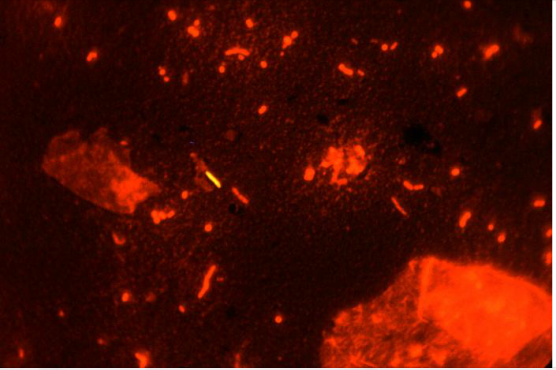
- Evaluate preliminary results using fluorescent microscopy
Decontamination
The lab I work at use the AlphaTec NAC-PAC® EA3 1 system. Samples are under digestion for 15 minutes, with vortex spin every 5 minutes. The NAC-PAC is also useful for breaking down mucous and sputum during the process.

Product photo
After digestion, apply the NPC-67 neutralizing buffer to prevent over-decontamination. The specimens are then put into the centrifuge (3000RPM for 15 minutes). Then, decant them to retrieve the pellets. At which point, use specialized pellet buffers to reconstitute the pellets.
Inoculation
The reconstituted and sterile specimens go on AFB slides2, MGITs3, and LJ slants4. For samples from surface of extremities, (arms, legs, etc.) they need a second set of MGIT and LJ. The second set would go into a cooler incubator to observe for possible leprosy.
The slides must go through heat fixing before taken out of the safety hood.



Look at all the different things we have to use.
Staining
Currently, the lab uses The Aerospray TB Series 25 to speed up the staining process. Like gram stain, it follows the steps of primary stain, decolorizer, then counterstain.
- Auramine-rhodamine (AR) stain
- Acid decolorizer
- Potassium permanganate
The machine could perform batch sizes from 1 to 30. But, 12 seems to be the optimal number. Anything after that, you would see noticeable quality decrease.
In my experience, manual staining tends to produce the best quality slides. But, they take much longer.

Didn't even get this until 2016
Results
Sometimes, you will see something in the slides. Sometimes, you won't. If you are lucky, you might see something like this among the debris.
Some educational material
The stains themselves do not disprove possible AFB infections. A positive stain result, however, warrants further actions. Clinicians and nursing stations need to be notified and infection control crew dispatched. This is also a type of infection the local and state government would like to know about. Depending on the source, there are more things to follow up.
For respiratory samples, the department forwards the resuspended pellets to molecular pathology. They would test them for Rifampin resistance in case it is tuberculosis.
For surface extremities, it's up to the clinicians to take precautions against leprosy.
For blood, clinicians could order more specific tests for Nocardia.
The MGITs and LJ slants will determine whether the patients have some sort of AFB infection. In order to rule them out, the cultures would have to go 42 days without any growth. Of course, the cultures should correspond to their positive slides. If not, there are more steps to take in troubleshooting.
To detect positive cultures, one method is using BD's MGIT system6. That's story for another day, which is a world in itself.
Absolutely loving these posts! A whole new very interesting world opening up :-)
Posted using Partiko Android
Glad someone is enjoying them.
Questo post è stato condiviso e votato all'interno del discord del team curatori di discovery-it.
This post was shared and voted inside the discord by the curators team of discovery-it
Congratulations @enforcer48! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPTo support your work, I also upvoted your post!
Vote for @Steemitboard as a witness to get one more award and increased upvotes!
That's a fascinating discussion. Not everyone would be comfortable working with the potential danger of these materials. Most people don't have the focus to be careful all the time (I don't), even if they have the expertise to conduct the tests.
I can't imagine people working with BSL-4 stuff.
Then, you are talking about stuff like Ebola, etc.
Will you be working with the Wuhan corona virus?
I think that will be handled by our molecular pathology department.
But, physicians will most likely order microbiology cultures on those patients too.
I haven't heard of cases in my area yet, but our leadership are preparing.