Medical microbiology, Neisserie / Microbiologia medica, Neisserie
Neisseria
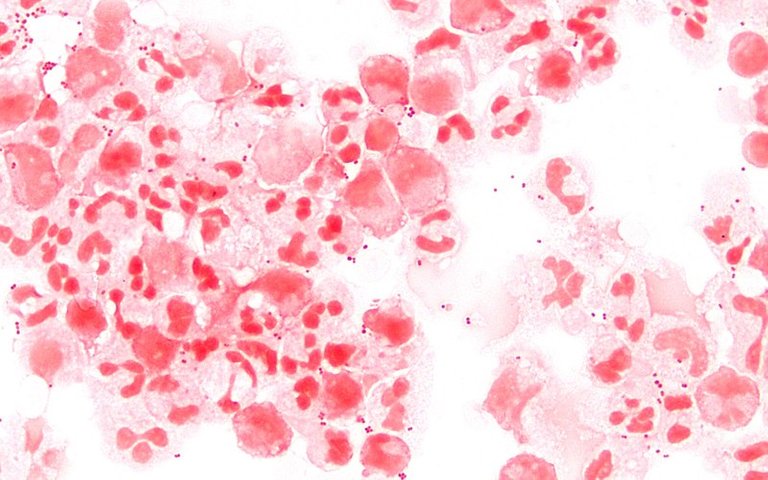
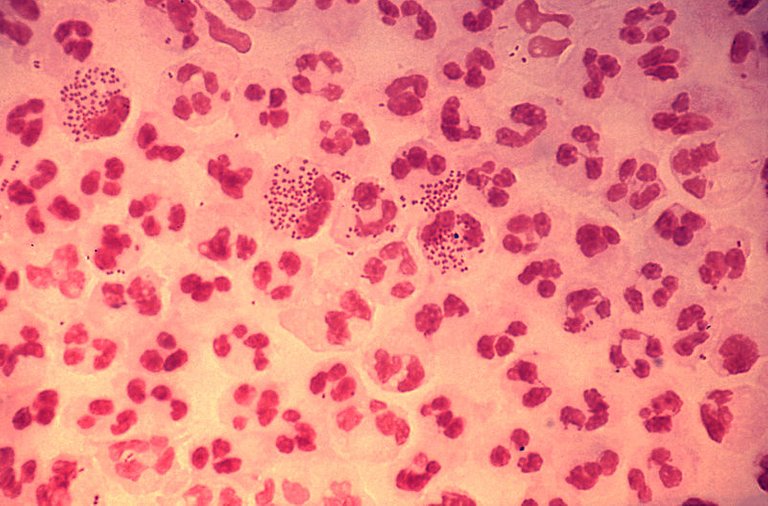
The Neisserie are Gram-negative coaches arranged in pairs, attached to each other for a large portion and for this reason called diplococchi coffee bean.
They are positive and aerobic catalase and oxidase bacteria.
They are equipped with a capsule which camouflages them and renders them pathogenic.
Their habitat is exclusively human: like the Haemophilus and the Pneumococcus, it is transmitted in human relations, for instance, by talking, through the droplets of flug, or through saliva exchange.
They grow well on both chocolate and blood Agar because they have no particular nutritional needs.
There are 2 types of Neisserie:
- Neisseria meningitidis : replica at the level of the oral cavity and upper respiratory tract and causes meningitis and sepsis.
- Neisseria gonorrhoeae: replication at the genital level causes gonorrhoea or blenoraggia, a sexually transmitted disease.
Neisseria meningitidis
The Neisseria meningitidis is characterized by the presence of proteins adhesives and opa and opc invaders, two antigens that allow the adhesion to mucous membranes and epithelia and the subsequent invasion.
It is also resistant to IgA because it has IgA-protease on its surface and is resistant to many antibiotics.
Its polysaccharide capsule is antiphagocytic, that is, it produces a substance that inhibits the formation of phagolisosome and therefore, if phagocyte, it can grow and reproduce within the phagosome formed. The capsule is of type b, in fact the bacterium colonizes and inflames the meninges.
The infection is endogenous: colonisation, asymptomatic, occurs in the oral cavity and in the nasopharynx (at least 10% of all of us have it in the oral cavity). If the bacterium is not stopped by the immune system, it has the ability to enter the circulatory stream or the CSF, causing meningitis preceded by very high fever, sepsis, intravascular coagulation, thrombi and petechiae. These events occur in a very short time and the infected person goes against death within one or two days, because the neisseria, previously, does not manifest itself.
Risk factors
- Any contact with a carrier.
- Immunity deficit.
- Active and passive smoking.
Pathological manifestation
The clinical cases of meningitis detected are around 200/250 per year throughout Italy and the mortality rate is very high. The subjects most affected are children and people with immunodepression.
As has been said, the colonization is asymptomatic and Neisseria hardly enters the cardiovascular system because it is blocked by the innate immunity but, when this does not succeed in stopping it, it can give rise to:
Meningitis: The first signs of meningitis are frontal migraine (because when the bacterium enters the chorioid plexus it inflames the cerebral ventricles that recall more liquor, spreading the meninges), nausea, vomiting, photophobia, fever, nuchal rigidity and in a few hours the patient goes into a coma and then reaches death. The phenomenology is immediate.
Expressions or septicemia. In less than 12 hours the patient may have a fatal sepsis caused by a disseminated intravascular coagulation that by purplish haemorrhages of the skin, extra blood vessel, diffuse micro-emboli and petechiae.
Other symptoms are vomiting, diarrhoea, very high fever, cardiovascular collapse and adrenal gland necrosis (very affected by the bacterium's invasion of the blood stream) and finally death.
Laboratory diagnosis
After taking a blood sample that is grown in specific liquid soils, a plasma gram is made or you can examine the CSF, which is usually cloudy. If the CSF is clear, the infection is not yet advanced and it is possible to study the bacterium with molecular techniques.
Isolation is done on blood Agar or chocolate Agar. A laryngopharyngeal swab is used to detect Neisseria meningitidis carriers. Neisseria can also be typed and evaluated by biochemical tests.

Neisseria gonorrhoeae
It is the second strain of Neisseria pathogenic to humans. The spread is only inter-human due to the presence of the bacterium in the genital organs (replicates well for example at the level of the urethra).
The Neisseria gonorrhoeae in vitro does not appear capsulated, but in vivo it has an antiphagocytic polysaccharide capsule that allows the possibility of growth within the polymorphonucleated leukocytes by not forming the phagolisosome.
It does not give meningitis.
Neisseria gonorrhoeae is equipped with:
- IgA-protease.
- Protein adhesives and pots opa and opc.
- Hair that give adhesiveness.
- Doors that allow the bacterium to adhere to the mucous membranes.
Grows well in Blood Agar or Chocolate Agar.
The gonococcus uses an additional mechanism of camouflage: it is characterized by molecules easily recognizable and attacked by the innate immunity so the bacterium has developed the ability to remove these molecules and store them in a "plasmid conservation" or "storing plasmid" and replace them with other molecules transcribed by another plasmid expression.
Neonatal gonococcal ophthalmia
Only hair-tipped skirts are virulent and transmission occurs through sexual intercourse; an infant can become infected if it crosses an infected delivery channel. The newborn baby taking the Neisserie gonorrhoeae on the face can have a strong eye infection and for this reason the tetracycline ointment is immediately applied to the eyes.

This infection is called neonatal gonococcal ophthalmia: the eye is totally swollen and closed and in the most serious cases it can lead to blindness.
The bacterium after being transmitted needs a point of a mucous membrane where there are pile receptors or opa or opc proteins to bind to the mucous membrane. The urethral mucosa, the uterine mucosa, the rectal mucosa, the conjunctiva and the oral cavity contain these receptors, the vaginal mucosa does not.
In women, if the infection occurs in the vagina, the disease is silent and asymptomatic: the bacterium moves from the neck of the uterus to the ovaries and in proceeding inflammation of the fallopian tubes, which heal and close, making the woman sterile.
In addition, chronic pelvic inflammation or "pid" (pelvic inflammatory disease) may occur, an annexiety in which the ovaries become inflamed and cause severe pain. The infected woman has the ability to transmit the Neisseria gonorrhoeae because it is present in the vaginal secretion.
More rarely the woman may be infected at the urethral level and show symptoms such as burning, continuous need to urinate, pus secretion. This allows you to identify the pathologist and proceed with the treatment.
The man, on the other hand, is always infected at the urethral level and shows symptoms such as localized burning, continuous need to urinate and loss of pus. In fact, when the penis of an infected patient is pressed down, the pus contained in the urethra comes out, which is called "early morning drop".
In a homosexual woman or man, the infection can be present in the anal mucosa and causes strong burns, continuous need to defecate, discomfort and pain in the infected area and formation of pus.
Depending on sexual habits, the Neisserie gonorrhoeae can also be located in the oral cavity.
Laboratory diagnosis
For the woman, an endocervical swab is made and possible DNA of Neisseria gonorrhoeae is searched for.
A slide of the pus and a Gram stain are made. If the sample to be studied is of anal or urethral mucosa, the bacterial growth is not pure because they are not sterile mucous membranes so the Thayer-Martin medium is used which contains the vancomycin to prevent the growth of Gram-positive bacteria, the colistin that does not grow Gram-negative especially those of the intestine, trimetropime and mistatin that are compounds active against many environmental bacteria to which the Neisseria gonorrhoeae is resistant.
The culture appears opalescent or pearly gray color that depending on how the light reflects many colors.
Prevention
Use a condom in sexual intercourse.
Since strains resistant to beta-lactam, tetracyclines, aminiglycosides, etc. have been isolated, it is important to have an antibiogram every time the bacterium is isolated. Third generation cephalosporins associated with a tetracycline or doxycycline are used to attack those forms of intracellular neisseries that grow in phagocytes.
Neisseria
Le Neisserie sono cocchi Gram-negativi disposti a coppie, adesi tra loro per una grande porzione e per questo detti diplococchi a chicco di caffe.
Sono batteri catalasi e ossidasi positivi e aerobi.
Sono dotati di una capsula che li mimetizza e li rende patogeni.
Il loro habitat è esclusivamente umano: come l’Haemophilus e lo Pneumococco viene trasmesso nei rapporti umani per esempio parlando, tramite le goccioline di flug ,o tramite scambio saliva.
Crescono bene sia su Agar cioccolato che su Agar sangue perchè non hanno particolari necessità nutrizionali.
Esistono 2 tipi di Neisserie:
- Neisseria meningitidis : replica a livello del cavo orale e delle vie respiratorie superiori e causa meningite e sepsi.
- Neisseria gonorrhoeae: replica a livello genitale causa la gonorrea o blenoraggia, patologia sessualmente trasmissibile.
Neisseria meningitidis
La Neisseria meningitidis è caratterizzata dalla presenza di proteine adesine e invasine opa e opc, due antigeni che permettono l’adesione alle mucose e agli epiteli e la successiva invasione.
Inoltre è resistente alle IgA poiché dotato di IgA-proteasi sulla sua superficie ed è resistente a moltissimi antibiotici.
La sua capsula polisaccaridica è antifagocitaria, ovvero produce una sostanza che inibisce la formazione del fagolisosoma e quindi, se fagocitata, può crescere e riprodursi all’interno del fagosoma formatosi. La capsula è di tipo b, infatti il batterio colonizza e infiamma le meningi.
L’infezione è endogena: la colonizzazione, asintomatica, avviene nel cavo orale e nel nasofaringe (almeno il 10% di tutti noi ce l’ha nel cavo orale). Se il batterio non è fermato dal sistema immunitario, questo ha la capacità di immettersi nel torrente circolatorio o nel liquor, causando meningite preceduta da febbre altissima, sepsi, coagulazione intravascolare, trombi e petecchie. Tali eventi si manifestano in tempi molto limitati e l’infetto va in contro a morte nel giro di uno o due giorni, poiché la neisseria, precedentemente, non da manifestazione di sè.
Fattori di rischio
• Eventuali contatti con un portatore.
• Deficit dell’immunità.
• Fumo attivo e passivo.
Manifestazione patologica
I casi clinici di meningite rilevati si aggirano sui 200/250 l’anno in tutta Italia e la mortalità è molto alta. I soggetti più colpiti sono bambini e persone con immunodepressione.
Com’è stato detto, la colonizzazione è asintomatica e la Neisseria difficilmente entra nel sistema cardiovascolare perché bloccata dall’immunità innata ma, quando questa non riesce a fermarla, può dare origine a:
Meningite: i primi segni della meningite sono emicrania frontale (poiché quando il batterio entra dentro il plesso corioideo infiamma i ventricoli cerebrali che richiamano più liquor, stendendo le meningi), nausea, vomito, fotofobia, febbre, rigidità nucale e in poche ore il paziente entra in coma per poi raggiungere la morte. La fenomenologia è immediata.
Sespsi o setticemia. in meno di 12 ore il paziente può avere una sepsi mortale causata da una coagulazione intravascolare disseminata che da emorragie violacee della cute, extra vaso di sangue, micro-emboli diffusi e petecchie.
Altri sintomi sono vomito, diarrea, febbre altissima, collasso cardiocircolatorio e necrosi delle ghiandole surrenali (molto colpite dall’invasione del torrente ematico da parte del batterio) e infine morte.
Diagnosi di laboratorio
Dopo aver eseguito un prelievo di sangue che viene coltivato in terreni liquidi specifici, viene fatto un Gram del plasma oppure si può esaminare il liquor, che solitamente è torbido. Se il liquor è limpido, l’infezione non è ancora avanzata ed è possibile studiare il batterio con le tecniche molecolari.
L’isolamento avviene su Agar sangue o Agar cioccolato. Per individuare i portatori di Neisseria meningitidis si effettua un tampone laringofaringeo. La Neisseria può inoltre essere tipizzata e valutata con test biochimici.
Neisseria gonorrhoeae
È il secondo ceppo di Neisseria patogeno per l’uomo. La diffusione è solo interumana data dalla presenza del batterio negli organi genitali (replica bene ad esempio a livello dell’uretra).
La Neisseria gonorrhoeae in vitro non appare capsulata, ma in vivo possiede una capsula polisaccaridica antifagocitaria che ne permette la possibilità di crescita all’interno dei leucociti polimorfonucleati non facendo formare il fagolisosoma. inoltre la capsula lo nasconde all’immunità.
Non dà meningiti.
Neisseria gonorrhoeae è dotata di:
• IgA-proteasi.
• Proteine adesine e invasine opa e opc.
• Pili che conferiscono adesività.
• Porine che permettono al batterio di aderire alle mucose.
Cresce bene in Agar sangue o Agar cioccolato.
Il gonococco utilizza un ulteriore meccanismo di mimetizzazione: esso è caratterizzato da molecole facilmente riconoscibili e attaccabili dall’immunità innata perciò il batterio ha sviluppato la capacità di togliere tali molecole e conservarle in un “plasmide di conservazione” o “storing plasmide” e sostituirle con altre molecole trascritte da un altro plasmide di espressione.
Oftalmia gonococcica neonatale
Solo i gonococchi provvisti di pili sono virulenti e la trasmissione avviene attraverso rapporti sessuali; un neonato può infettarsi se attraversa un canale del parto infetto. Il neonato prendendo la Neisserie gonorrhoeae sul viso può avere una forte infezione oculare e per questo viene immediatamente applicata sugli occhi la pomata alla tetraciclina.
Tale infezione si chiama oftalmia gonococcica neonatale: l’occhio è totalmente tumefatto e chiuso e nei casi più gravi può portare a cecità.
Il batterio dopo essere trasmesso necessita di un punto di una mucosa in cui ci siano dei recettori dei pili o delle proteine opa o opc per legarsi alla mucosa. La mucosa uretrale, la mucosa uterina, quella rettale, la congiuntiva e il cavo orale contengono tali recettori, quella vaginale no.
Nella donna, se l’infezione avviene a livello della vagina, la patologia è silente e asintomatica: il batterio trasloca partendo dal collo dell’utero per poi arrivare alle ovaie e nel procedere infiamma le tube di Falloppio, che cicatrizzano e si chiudono, rendendo la donna sterile.
Inoltre può manifestarsi un’infiammazione pelvica cronica o “pid”(pelvic infiammatory disease), un’annessite in cui le ovaie si infiammano e provocano un forte dolore. La donna infetta ha la capacità di trasmettere la Neisseria gonorrhoeae poiché è presente nel secreto vaginale.
Più raramente la donna può essere infettata a livello uretrale e manifestare sintomi quali bruciore, continua necessità di urinare, secrezione di pus. Ciò permette di individuare la patologa e procedere con la cura.
L’uomo invece è sempre infetto a livello uretrale e manifesta sintomi quali bruciore localizzato, continua necessità di urinare e perdita di pus. Infatti quando il pene di un paziente infetto viene premuto fuoriesce il pus contenuto nell’uretra, che viene detto “goccia del buon mattino”.
Nella donna o nell’uomo omosessuale l’infezione può essere presente nella mucosa anale e provoca forti bruciori, continua necessità di defecare, malessere e dolore nella zona infetta e formazione di pus.
A seconda delle abitudini sessuali le Neisserie gonorrhoeae possono essere localizzazione anche a livello del cavo orale.
Diagnosi di laboratorio
Per la donna si effettua un tampone endocervicale e si va a cercare DNA eventuale di Neisseria gonorrhoeae.
Viene effettuato un vetrino del pus e una colorazione Gram. Se il campione da studiare è di mucosa anale o uretrale, la crescita batterica non è pura poiché non sono mucose sterili perciò viene utilizzato il terreno di Thayer-Martin che contiene la vancomicina per non far crescere batteri Gram-positivi, la colistina che non fa crescere Gram-negtativi specialmente quelli dell’intestino, trimetropime e mistatina che sono composti attivi verso tanti batteri ambientali ai quali invece la Neisseria gonorrhoeae è resistente.
La coltura appare opalescente ovvero di colore grigio perlacea che a seconda di come gira la luce riflette tantissimi colori.
Prevenzione
Usare il profilattico nei rapporti sessuali.
Siccome sono stati isolati ceppi resistenti ai beta-lattamici, alle tetracicline, agli amminiglicosidi, etc. è importante fare l’antibiogramma ogni volta che il batterio viene isolato. Per attaccare quelle forme di Neisserie intracellulari che crescono nei fagociti si utilizzano le cefalosporine di terza generazione associate ad una tetraciclina o alla doxicillina.
Fonti/Souces
Meningite
Gonorrea
Immagini/Pictures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Questo post è stato condiviso e votato dal team di curatori di discovery-it.
This post was shared and voted by the curators team of discovery-it
This post was shared in the Curation Collective Discord community for curators, and upvoted and resteemed by the @c-squared community account after manual review.
@c-squared runs a community witness. Please consider using one of your witness votes on us here
Random tidbit:
I have only come across one patient positive for gonorrhea this year during my shift.
really very strange! we invent the strangest stories about how was taken the gonorrhea, the most popular is that they went to swim in the pool and the bath of the autogrill
There are crazy stories, then there are strange orders by doctors.
One of the gonorrhea culture ordered, it was from a patient's knee. It was negative, but my coworkers and I chuckled because that would have been a strange kink.
From the knee? omg this is crazy
It was super weird, but that's what the doc wanted, so...
Congratulations @riccc96! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPDo not miss the last post from @steemitboard:
This content has earned some GEEK. 50.000 GEEK tokens has been transferred to your steem-engine.com account.
Geek Rewards (GEEK) is a steem engine token that rewards content creators for their geeky contributions to the community.
Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
Please join us on discord.