General description of mechanical ventilation use and general care
Breathing is composed of the inhalation or inspiration phase and the exhalation or expiration of this first is responsible for oxygenating each cell of our body, to favor the production of energy and the second aid to lymphatic drainage and detoxifies the body, with the elimination of carbon dioxide.
When our body does not receive oxygenation for a few minutes through the breathing process, for example, the brain cells begin to die and in the same way it happens with the heart, the kidneys and thus with all the organs of the human body, which puts Imminent life risk. Breathing is our first source of energy, if we have a good oxygenation the organism will have physical, psychic vitality.
Breathing is so important that we could spend days without feeding ourselves well, without being able to sleep, without drinking water, but not without breathing, since with only 5 minutes of absence of this it would mean death.
Running out of breath for a moment or having difficulty breathing is one of the most common reasons to go to a health center and this in turn becomes a real challenge for professionals who provide health, because if we can not solve with therapeutic measures and pharmacological, we will require technology such as The Mechanical ventilator, to replace the function of breathing in a patient who cannot do it alone.
If we do not have the technology to give a patient breaths we can do it through a manual insufflation bag, which would be a very nonspecific procedure since you cannot supply desired pressures and volumes, and This act generates great wear on the professional who performs it for hours and in most cases instead of being beneficial for the patient is harmful favoring death
Creation of the Mechanical Fan?
Perhaps many consider that mechanical ventilation is a current practice but has its beginnings in 1543 with the first experimental application of ventilation thanks to the doctor Andrés Vesalio, for the moment it was not considered of importance and that was when later centuries the investigations were resumed in relation to mechanical ventilation and the well-known steel lungs were born thanks to the Alfred F. Jones ventilation tank that allowed to maintain respiratory function through the use of negative pressure.
From there, many prototypes of mechanical ventilation devices emerged, such as the one created in 1902 by Ernst F. Sauerbruch, which consisted of a negative or low pressure chamber that prevents lung collapse was widely used at that time for surgeries in which should open the chest.
But the real enhancement in the management of mechanical ventilation arises from the year 1938 where intermittent positive pressure is used, this modality is very similar to those we know today.
Thanks to this technology that was available at the time in 1952 in the Poliomyelitis epidemic in Denmark, Mechanical Ventilation was used to a large extent and since then year after year has been created devices with high technology and precision to promote health from the patients.
What is the Mechanical Fan?
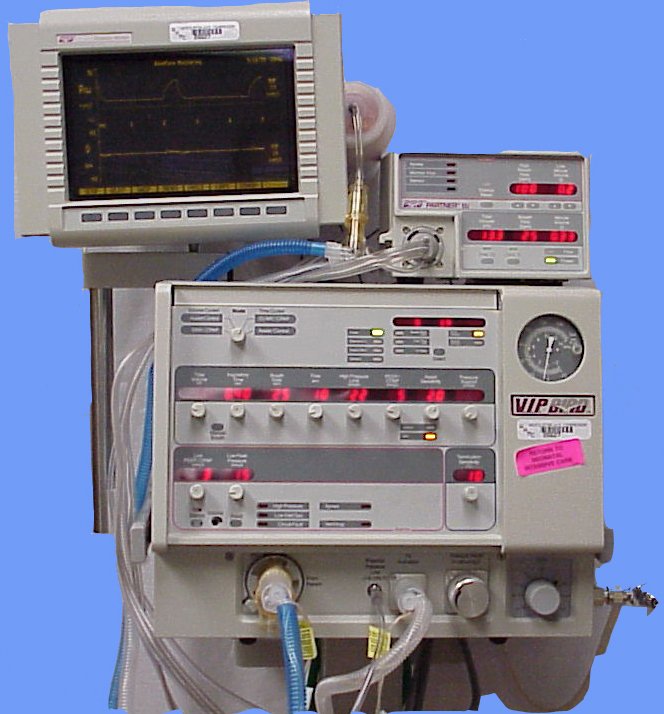
It is a therapeutic measure to replace the respiratory functions of a patient when he cannot do it on his own, the mechanical ventilator is a solid device, built with high technology and precision made of metal and plastic, with electronic cards, which detect and send signals to the control panel of this device (Touch screens or Pressure Clocks).
In order for this to be connected to a patient, it is necessary to resort to a medical procedure called Orotracheal Intubation, which consists in the placement of a plastic tube from the external medium to the trachea and through this tube which connects the mechanical fan connections for operation.
How Gas Mixing Works (oxygen and Carbon Dioxide) in the Mechanical Ventilator?
Inside the mechanical fan we will find a device called Blender which is a medical air mixer (oxygen and compressed air), this makes it possible to play with the concentration of oxygen that can be supplied to a patient already which allows to supply in a range of 21% to 100% in the inspired gas.
This process occurs through an electric valve (solenoid) where it performs an opening and closing according to the inspiration or expiration phase, for a proper function of it the pressure of the medicinal gases must be constant, so there must be a team monitoring the pressure of these gases
Parts of a Mechanical Fan
In its front part we will find the control panel or interface system, through this you can set parameters for the patient according to their pathology, from this device we will find two connections one that comes out and the other one that enters as they are the inspiratory and expiratory valve, we will also find a connection for the proximal flow sensor, and to fog if the equipment allows it.
On the back of the mechanical fan there are connections, such as the electrical source and medicinal gases. There are also ports to computer connections for data extraction, as well as for software and scanner updates in fault detection and mechanical fan repair.
Mechanical Fan Connections
The first of this is the inspiratory line where the air pressure of the ventilator duly programmed in a set time, flow and pressure is sent.
The second is the expiratory line where the air exhaled by the patient exits through a valve that removes it to the environment.
Both lines are joined, although each of them fulfills its function defined by the parameters established during the operation of the fan, so the flow sensor will be responsible for verifying if the preset pressures or volumes are correct.
Mechanical Fan Alarm System
A mechanical fan like any other technological device used in the health area uses an alarm system that the equipment manufacturer uses automatically, such as the lack of supply of medical gases, electricity or disconnection of the patient due to loss of pressure, will activate the alarm.
Other of these alarms are adjustable by the doctor when the patient connects, for example the high and low airway pressure, the high and low minute volume, the high respiratory rate and the apnea period.
This alarm system makes them very safe equipment and facilitates care in patients with respiratory conditions.
Indication of mechanical ventilation
There are numerous reasons for using this device but among the most frequent we have:
Apnea (absence of breathing)
Severe hypoxemia despite adequate oxygen therapy
Hypercapnia
Respiratory work (> 35 breaths per minute)
Vital capacity (<10 ml / kg or inspiratory force <25 cm H2O
Fatigue of the respiratory muscles (exhaustion)
Deterioration of level of consciousness
Respiratory muscle dysfunction
Thoracic wall alterations
Neuromuscular disease
Decrease of ventilatory impulse
Increased Airway Resistance
Refractory hypoxia
Positive Pressure Accuracy at the end of the expiration.
Excessive respiratory work
To allow sedation and neuromuscular blockade
To decrease myocardial oxygen consumption
To reduce Intracranial Pressure in neurosurgery.
To prevent atelectasis
The use of mechanical ventilation has some physiological objectives:
Maintain, normalize or manipulate the gas exchange
Provide adequate ventilation or at the chosen level
Improve arterial oxygenation
Increase lung volume
Open and distend airways and alveoli
Reduce respiratory work
Improve hypoxemia
Correct respiratory acidosis
Relieve breathlessness and discomfort
Prevent or remove atelectasis
Reverse fatigue of respiratory muscles
Allow sedation and neuromuscular blockade
Decrease the volume of systemic and myocardial O2
Brief anatomical and physiological description of the breath
The thoracic cavity is structured so that it has the ability to distend according to the air pressure it receives, and all this thanks to anatomical details such as bone, cartilage, blood vessels, muscles and viscera, which allow this property.
The thorax can be limited by different structures, such as the Antero-posterior and lateral limit by the thoracic wall: a semi-rigid structure composed of ribs, sternum vertebrae and intercostal muscles. In turn in the Lower Limit. the diaphragm and in its Upper Limit the cavity is closed by connective tissue and vascular structures.
Likewise, the rib cage internally is divided primarily into mediastinum that includes the esophagus, trachea, heart, aorta and other vessels and secondarily into pulmonary cavities represented by the lungs.
These are connected to the mediastinum through the pulmonary Hilio. Each of the cavities is limited by the chest wall, diaphragm and mediastinum.
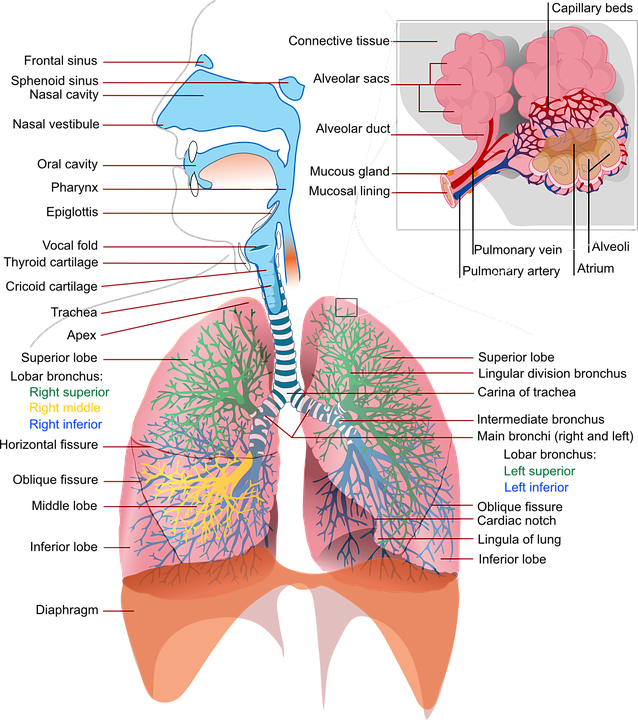
Both lungs are covered by a membrane called Pleura and this in turn is divided into visceral (membrane that covers the lungs), and parietal (membrane which covers the chest wall and the diaphragm muscle by its upper face).
These structures, as they are the visceral and parietal pleura are intimately linked but inside it has a virtual space or pleural space where there is little liquid that lubricates the movement of the lungs inside the thorax during the ventilatory cycle Within this space there is a negative pressure that acts as a vacuum, which prevents the lungs from collapsing.
In this intrapleural space we talk about negative pressure, taking as reference that the atmospheric pressure is equal to zero; so all pressure less than atmospheric is considered negative; therefore this negative pressure acts by expanding the lung and if the pressure is positive it collapses
Breathing means much more than just transporting oxygen to the lungs and removing carbon dioxide through expiration.
The ventilatory cycle consists of the phase of inhalation or inspiration and exhalation or expiration thus managing to oxygenate the cells of the human body, favoring the production of energy as well as contributing to the lymphatic drainage and detoxification of the organism, with the carbon dioxide removal.
Breathing is so important that we could spend days without feeding ourselves, without sleeping, but not without breathing, since with only 5 minutes of absence, brain death is sentenced and therefore the rest of the body .
The negative pressure that exists in the intrapleural space, helps keep the lung distended. This pressure in turn varies according to the phase of the ventilatory cycle that is found, end of expiration (- 5 Cm H2O) or during inspiration (- 8 cm H2O).
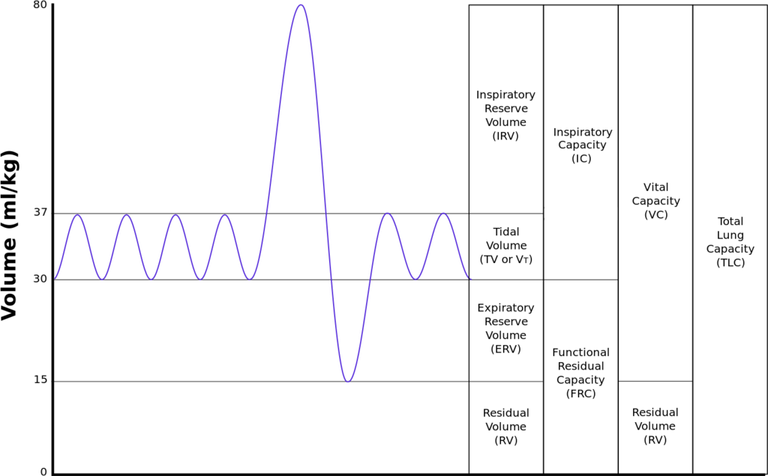
Within the physiological framework of respiratory function it is important to know the different volumes and capacities that occur in the breathing process, among them we have:
Tidal Volume (VC):
It is the amount of air that enters and leaves the lungs, but is not exchanged.
Expiratory reserve volume (VRE):
It is the amount of additional air that can be exhaled through forced expiration.
Residual volume (VR):
The amount of volume of air left in the lungs and respiratory tract after forced expiration.
Inspiratory capacity (CI):
It is the amount of air that can be breathed from a normal expiration, achieving the maximum distention of the lungs, we can say that it is obtained from the sum of the tidal volume and the inspiratory reserve volume. CI = VC + VRI
Functional residual capacity (CRF):
It is the amount of air left in the lungs after normal expiration. And it is obtained by adding the expiratory reserve volume and the residual volume. CRF = VRE + VR
Vital capacity (CV):
It is the amount of air possible to expel from the lungs after having completely inspired. It is obtained from the sum of the tidal volume, the inspiratory reserve volume and the expiratory reserve volume. CV = VRI + VC + VRE
Total lung capacity (CPT):
It is the amount of air that can be obtained in the respiratory system, after a maximum voluntary inhalation. We obtain it with the sum of the tidal volume, inspiratory and expiratory reserve volume plus residual volume. CPT = VC + VRI + VRE + VR
Conditions for the installation of the ventilatory support
To establish mechanical ventilation in a patient, a series of conditions must be taken into account since this will allow choosing the ventilator and parameters appropriate to the clinical condition of the critically ill person among which we have:
1.Choose the mechanical fan mode.
2.It must start with a FiO2 of 100%.
3.Perform an arterial gas test to evaluate the parameters established in the mechanical ventilator and its functionality in the patient.
4.Calculate the tidal or tidal volume VC / VT of 8-10 ml / kg
5.If the pathology is Adult Respiratory Distres Syndrome, the following constant 5-8 ml / kg is used to calculate the tidal volume.
6.Choose respiratory rate and minute volume depending on the patient's clinical situation.
7.Establish positive pressure at the end of expiration (PEEP) to improve oxygenation and reduce FiO2. Being this No> 15 cm H2O.
8.Modify flow and frequency to avoid turbulence and alveolar air entrapment.
9.Administer analgesia, sedation, relaxation and posture of the patient according to the oxygen saturation presented by the patient.
10.Constantly monitor and record the Blood Pressure, Heart Rate, oxygen pressure and blood O2 saturation (PaO2-SaO2), as alarm values for any unwanted effects that may occur
Mechanical fans have different forms of cycling that according to the pathology will determine which one to use:
1.Cycled by volume (VT)
2.Cycling by airway pressure
3.Cycled for time
4.Cycled by decrease in inspiratory flow
Once the classification of mechanical ventilation by cycling is determined, the ventilation mode is chosen as the device will work, thus existing:
1.Volume control.
2.Control pressure.
3.Assisted / controlled (AC)
4.CMV (Controlled mechanical ventilation).
5.SIMV. (Synchronized intermittent mandatory ventilation)
6.CPAP. (Continuous positive pressure).
7.High frequency ventilation.
8.Ventilation with pressure support (PSV).
9.Ventilation with pressure release (APRV).
10.Mandatory minute ventilation (MMV).
11.Independent pulmonary ventilation (ILV).
General care in patients connected to mechanical ventilation
For the care of patients with mechanical ventilation, a series of more specific actions are carried out that help the patient gradually improve his condition and at the same time allow the nurse to obtain greater patient monitoring.
General Interventions:
1.Vigilance of vital signs.
2.Pulse oximetry (pulse oximeter).
3.Rx of the post-intubation thorax to assess the location of the tube and fixation of the tube at the corner of the mouth.
4.Arterial gasses at the beginning of the Mechanical Ventilation and in regular periods to take conduct in the ventilatory parameters.
5.Monitor respirator curves.
6.Intracranial pressure in patients with neurosurgery and cardiac output.
7.Constantly evaluate renal function and liver function
8.Aspiration of secretions by orotracheal tube and nostrils.
9.Preventive measures in the reduction of pneumonia associated with mechanical ventilation.
10.Oxygen toxicity
11.Psychological complications
12.Hypotension associated with Mechanical Ventilation
13.Auto-PEEP
References
Reference 1
Reference 2
Reference 3
Reference 4
Reference 5
Reference 6
Reference 7
Reference 8
Reference 9
{kind=link}
{kind=link}

@felixrodriguez
Nurse Specialist in Patient Care in Critical Status.
Nurse Specialist in Patient Care in Critical Status.
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.
To listen to the audio version of this article click on the play image.

Brought to you by @tts. If you find it useful please consider upvoting this reply.