Medical microbiology, Clostridia, Tetanus, and Botulinum / Microbiologia medica, Clostridi, Tetano, e Botulino
Clostridia
readers are warned that some of the images in the article may be strong
General characteristics
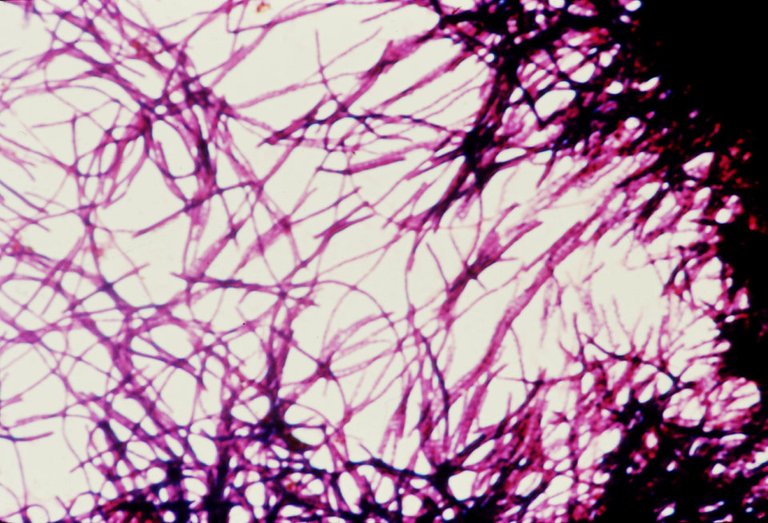
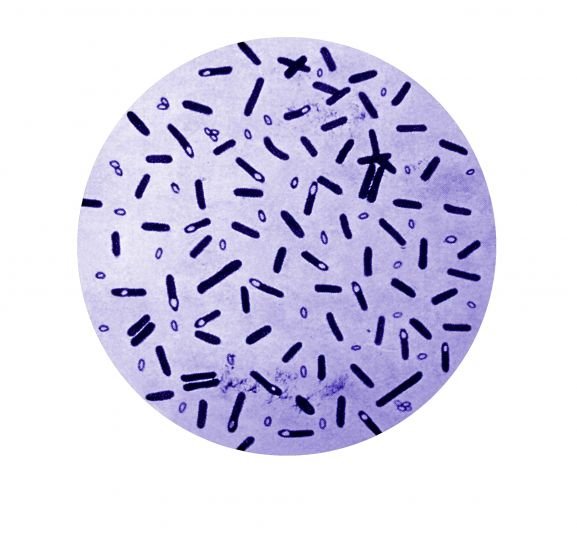
Clostridia are Gram positive bacilli, sticks of varying sizes, ubiquitous environmental but that can only be present in the environment in an inert form. Within this family we recognize a few species that are responsible for extremely serious diseases in humans.
The fact that they are ubiquitous but inert in the environment depends on their peculiar characteristics, possessed by a few species among the bacteria of human competence. One of these is sporigenicity, a characteristic that makes these bacteria capable of living in many adverse conditions, even in the most disparate environments and the other is anaerobic, a condition not easily found in environments related to life. As for the latter, some clostridia are strictly anaerobic, others are more aero-tolerant.
A microenvironment suitable for the active replication and metabolism of these bacteria will therefore be an oxygen-free environment, while almost all environments will not be adequate for clostridic proliferation and therefore the survival of these is linked to a presence in the form of spore, a form of survival of the metabolically inactive bacterium.
Contamination can occur through these spores: most of the time no infection or colonization can originate from this because we will not present clostridium with a suitable environment for proliferation, but it can happen that micro-aerophilic or anaerobic zones are created in the body (for example ischemic zones that can occur after traumas where there is no longer vascularization) and therefore become suitable zones to be colonized. Therefore, the fermentative metabolism of these bacteria is active only in extremely reducing conditions because, being anaerobic, they are not able to use oxygen as an electron donor.
Habitat
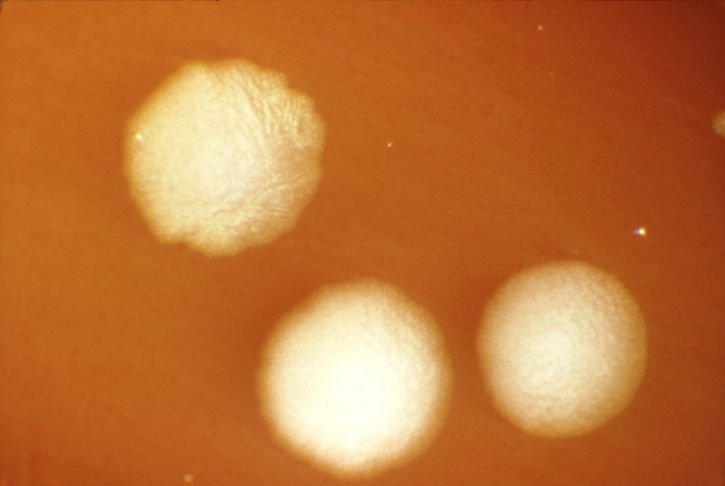
Ubiquitous environment: soil, sewage, aquatic environments with high organic content.
Organisms: apathogenic colonization by a series of clostridia, including those pathogenic to humans, of the intestines of mammals, an anaerobic microenvironment where areas of very important fermentation are created by commensal and resident flowers.
This generates a suitable reducing environment and an anaerobic condition suitable for the proliferation of clostridia. In particular, these bacteria colonise the intestines of ruminants.
The proliferation of clostridia leads to the generation of numerous spores which, spreading in the surrounding environment, can lead to its contamination. This creates environments with a high risk of contamination, such as rural environments, racetracks, stables, stables, etc..
The spores of these bacteria are resistant to
Chemical disinfectants
Exposure to ultraviolet rays
Boiling temperatures for a certain period of time
They are only destroyed by a standard autoclaving process (121° C for 15 minutes)
Sporulation
The spore is generated when the bacterium makes the sensing of adverse conditions (i.e. the presence of oxygen). This triggers a process of gene regulation involving 200/300 genes leading to the generation of an abnormal daughter cell, not resulting from a binary split, different from the mother, who will die after giving her daughter the characteristics that make her inert and resistant.
A series of resistant protective structures will be generated, within which there will be a dehydrated content, which contains inactive enzymes and nucleic acid. At the right time the spore (which is the equivalent of the seed in the plants) will have to germinate giving rise to a new bacterium with an intact nucleic acid and enzymes that will restart the metabolism and that will lead to the rupture of the leathery layers, which make the spore resistant to a series of environmental attacks.
Pathogenic power
The pathogenic power of all clostridia of medical interest lies not only in their extreme resistance to the environment, but also in the production of toxins, which give intoxications more or less important in the condition of germination, ie when the bacterium will be in optimal condition to be able to proliferate.
In most cases, man is intoxicated not directly by the bacterium, but by the toxic product acquired as a pre-constituted by situations in which the bacterium has been able to proliferate and give rise to its pathogenic products.
The two bacterial strains most canonically associated with disease are clostridium botulinum, the etiological agent of botulism, and clostridium tetani, the etiological agent of tetanus. Both are deadly diseases mediated by the production of two exotoxins which are respectively the botulinum toxin and the tetanus toxin. As far as clostridium tetani is concerned, the vaccine is mandatory in the first months of life because it is extremely widespread in the environment and it is very easy to acquire it, unlike botulism, which is rarer.
The toxins produced by clostridia are all binary toxins A-B toxin, in which one region of the toxin is responsible for binding the receptor (B), while the second is the real active zone of the toxin (A). The toxin enters the target cells that it identifies through the binding region and then releases within the active site the fragment that will interact with different targets depending on the type of toxin.
Clostridium Perfrigens
It is a capsulated bacterium, Gram positive, ubiquitous component of the flora of the gastroenteric tract and sometimes also of the vaginal flora. It is an important pathogen because, like all clostridia, it produces exotoxins that can reach even areas far from the site of infection, but it is the only one of this family that acts as a pathogen even producing degrading enzymes (or histiolytics, or hydrolytes) that guarantee a strong invasive power, regardless of the action of the exotoxins.
It has many virulence factors and produces numerous toxins including phospholipase C, which breaks down cell membranes, killing the cells that come into contact with it, and has a necrotizing activity at tissue level, thus becoming a determining factor in the onset of gaseous gangrene (or tissue myonecrosis induced deep tissue).

Tissue necrosis promotes further proliferation of this anaerobic bacterium. Another important toxin is tetatoxin, which is an hemolysin; then there are hyaluronidases, proteases, collagenases and cytolytic toxins that give it a high power of tissue invasiveness. It also produces a very aggressive enterotoxin which alters the permeability of the ileum and blind membranes and has an important inflammatory function, degrading the functions of the enterocyte.
Pathogenesis
It causes cellulitis and bundles (also found in Staphylococci and Streptococci) and leads, in its version of greater ability to attack, to a disease called gaseous gangrene or tissue myonecrosis induced deep tissue, usually as a result of serious wounds such as war wounds or traumatic crushing wounds (in which are created ischaemic zones of anaerobic disease where the bacterium can replicate).
It is called gaseous gangrene because under optimal conditions this bacterium has a high replication activity, a tumultuous metabolism, which produces as a result of fermentation a large amount of gas that accumulates in bubbles and produces crackles. The only way to eradicate the problem is to amputate or remove the affected area, to avoid that the infection increasingly involves a greater amount of tissue.
It can also cause necrotizing endometritis, because being also part of the vaginal flora, in conditions of abortion, it can happen that the vaginal flora itself, containing this clostridia, goes to infect necrotic tissues that are formed after abortion (even spontaneous). Another quite characteristic disease is due to the presence of the bacterium in the intestinal tract, which causes food poisoning, if the toxin is taken from the outside or a necrotizing enteritis, if the bacterium colonizes the intestine and replicating produces enterotoxins inside the body.
Treatment
Infections with clostridium botulinum and clostridium tetani are replication-independent, i.e. there is no need for replication of the bacterium to give disease, but the only factor of virulence is the toxin, so antibiotic therapy would have no effect. Where, on the other hand, part of the pathogenesis is the replication of the bacterium, antibiotic therapy is important and clostridium perfrigens is generally sensitive to penicillin.
The other important therapy (also of prevention) is the hyperbaric chamber, which gives an exogenous tissue hyperoxygenation that favors the metabolic slowdown of the proliferation of Perfrigens and the maintenance in life of the affected tissues, where possible. This treatment, associated with antibiotic therapy, limits the progression of the disease. Clostridium Perfrigens, like botulism, is quite rare.
Clostridium Botulinum
Characteristics
It is a very narrow anaerobic that produces neurotoxins that lead to paralysis. Clostridium botulinum is taken from the environment that has been contaminated by faeces from the intestines of ruminants; the spores are deposited on plants or are present not only in the intestines but also in the tissues of animals and, therefore, we take them by eating vegetables or meat. An example of a food from which we can contract clostridium botulinum is the aerobic tomato paste, in which the bacterium can proliferate, but this is not the phase in which the toxins are produced. Toxins are generally produced in the pre-sporiginal phase, and therefore, in the previous example, at the time when the preservative is exposed to air. The bacterium, feeling the presence of oxygen, before becoming spore, releases toxins.

Pathogenesis
Botulinum toxin is the most powerful natural poison we know today (250mg would be enough to exterminate the entire world population).
This toxin targets neuromuscular plaques. Usually in them, the excitatory motor neuron releases the excitatory neurotransmitter (e.g. acetylcholine) through the vesicles by contracting the muscle fibres, then the inhibitory motor neuron through the inhibitory neurotransmitter (e.g. GABA) releases the muscle.
Botulinum toxin specifically inhibits the release of acetylcholine from presynaptic bladders, resulting in flaccid paralysis, as muscle fibres will no longer contract, sometimes permanently. Botulinum toxin is also used to reduce wrinkles, but its use can limit facial expression.

The effect of this toxin is extremely long-lasting. If the systemic spread of this toxin cannot be contained, especially in the upper part of the body, it can lead to death by blocking the diaphragm and heart muscle (thus affecting both voluntary and involuntary muscles).
Botulinum toxin consists of 8 isoforms (A,B,C-α,C-β,D,E,F,G) that act on the vesicular system, targeting different moments of secretion.
- The isoforms B,D,F and G cut synaptobrevin
- C isoforms cut syntaxin and SNAP-25 protein
- The isoforms A and E cut the SNAP-25 protein and prevent the release of acetylcholine, acting on molecules involved in the fusion of the vesicle acetylcholine at the nerve end.
Classification
There are 3 types of botulism
Classic botulism: explained above
Infant botulism: If spores reach an intestine where there is not yet a consistent resident flora, they can germinate and give an intestinal toxin infection, which is often self-limiting and causes severe intestinal problems. The toxin almost never enters the circulation causing a systemic disease.
Wound botulism (rare): very similar to wound tetanus
Treatment
The vaccine is difficult to obtain and we can contain botulism satisfactorily even by simply preventing it.
It is important not to give honey to children under one year of age to avoid infant botulism.
Clostridium Tetani
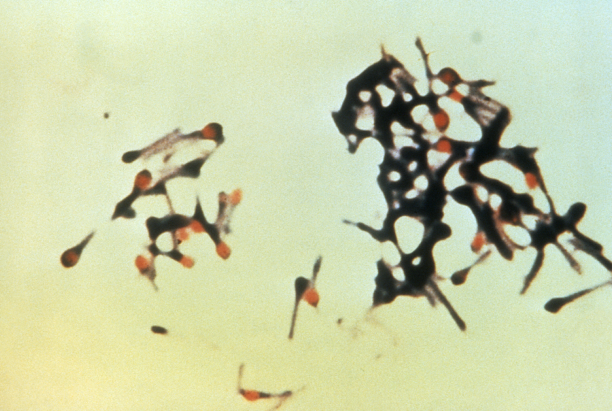
It is a clostridium strictly anaerobic, which in culture we can not see as a stick, but as "drumstick" because it is so anaerobic, that it is always in condition to sporulate.
Pathogenesis
The pathogenesis of tetanus is linked to the single tetanus toxin, because the disease caused by wound infection is the most common form and is called wound tetanus. Every time we infect a wound with tetanus spores we are at a very high risk of contracting tetanus (a rare event for Clostridium botulinum) and if we did not control the disease with the vaccine it would be extremely widespread.
It is easy to become infected with tetanus spores by coming into contact with rusty iron, which releases splinters causing a torn-contused wound where a microenvironment of tissue necrosis is created within which the bacterium can replicate. When contamination is suspected, it is advisable to incise the injured area and bleed to oxygenate the tissue and prevent disease progression.

Being the bacterium strictly anaerobic in vivo it will tend almost immediately to sporulate, producing first the two toxins
A tetanolisin, which does not cause any tissue damage
The tetanospasmine, the only true virulence factor of clostridium tetani
This is an A-B toxin and its active area is a protease that cuts synaptobrevin, acting at the muscle level as in botulism. The binding side of tetanospasmine, however, finds its receptor not on the excitatory motor neuron (as in botulism), but on the inhibitory motor neuron, which will not secrete the inhibitory neurotransmitter (GABA or glycine). This will lead to tetanus contraction, a muscle hyper-contraction called tetanus spasm of the muscle, which fails to relax.
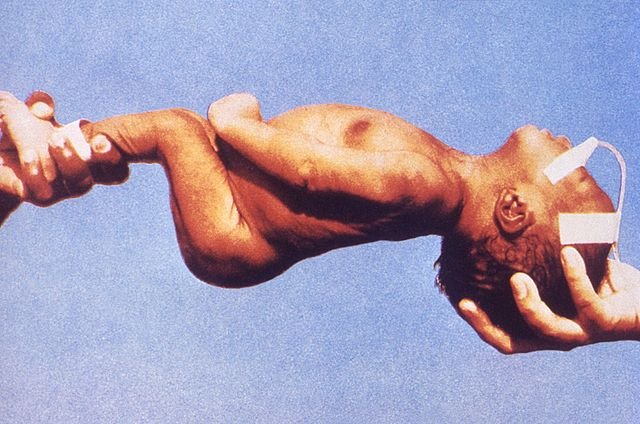
The result is a spastic paralysis (not flaccid as in botulism) that, in the terminal phases, leads to contraction of the dorsal muscles, resulting in bending of the back, while one of the first signs is the risus sardonicus, contraction of the facial muscles that leads to this expression similar to a smile.
When the toxin spreads, the disease is called generalized tetanus.
When, on the other hand, we come into contact with a minimum amount of spores, tetanus can be defined as localized, since the toxin that will be produced will only be able to act at the level of the local muscle and will not reach the circle spreading to the whole organism. Localized tetanus generally precedes generalized tetanus, so a careful history should prevent it
.
Neonatal tetanus is very frequent, widespread in countries with a low level of development, where there are parts in poor hygienic conditions and where there may be an infection of the umbilical cord, which must go into necrosis to create the stump, causing a region with a very high risk of tetanus. Mortality is very high.
Treatment
The tetanus vaccine is one of the oldest vaccines we use, widely used. It is very safe and is based on our body's ability to generate antibodies that permanently inhibit the possible presence of toxin in the body.
The tetanus toxin is a strongly immunogenic protein, which remains so even if its active sites are modified by chemical treatments, which change the conformation making them inactive, but maintain unchanged the immunogenic regions.
The toxin thus modified is called anatoxin or toxoid and can be injected into the subject, where it will give rise to a reaction that will produce neutralizing antibodies, which will be able at the time of the presence of the real toxin in the body to go and prevent the deleterious effects that it can produce. Vaccination is mandatory at the infant level (at the third month of life) and it is strongly recommended to make subsequent boosters to keep the number of antibodies above a certain level.

Therapy
In patients over 60 years of age, the incidence increases dramatically, partly because then the vaccine was not widespread, but mainly because the immunity acquired in childhood, without ever recalling the vaccine, at some point is lost.
If you were not covered by vaccination, at the first symptoms (often it is localized tetanus) you can go to treat with preformed antibodies, which neutralize the toxin. These antibodies can be administered on site intramuscularly, from where they enter the circulation.
These are usually hyperimmune sera from recently vaccinated subjects. These subjects produce a large amount of antibodies, which are collected with the serum and are purified from it the immunoglobulins against tetanus tetracycline that are injected into subjects who have not been vaccinated. However, these sera must be used with caution as they are blood products.
A passive immunoprophylaxis is therefore carried out when there is a high risk of contracting disease or a passive immunotherapy when tetanus is already present and this therapy serves to prevent its evolution. Antibiotics have no effect on the tetanus toxin, they are only able to make the bacterium sporulate (useless or even harmful reaction).
Clostridi
si avvisano i lettori che alcune immagini presenti nell'articolo possono essere forti_
Caratteristiche generali
I clostridi sono bacilli Gram positivi, bastoncellari di dimensioni variabili, ambientali ubiquitari ma che possono essere presenti nell’ambiente solo in forma inerte. All’interno di questa famiglia riconosciamo poche specie che sono responsabili di malattie estremamente gravi nell’uomo.
Il fatto che nell’ambiente siano ubiquitari ma inerti, dipende dalle loro caratteristiche peculiari, possedute da poche specie tra i batteri di competenza umana. Una di queste è la sporigenicità, una caratteristica che rende questi batteri capaci di vivere in molte condizioni anche avverse, nei più disparati ambienti e l’altra è l’anaerobiosi, una condizione non facilmente riscontrabile negli ambienti collegati alla vita. Per quanto riguarda quest’ultima alcuni clostridi sono strettamente anaerobi, altri sono più aero-tolleranti.
Un microambiente adatto alla replicazione attiva e al metabolismo attivo di questi batteri sarà dunque un ambiente privo di ossigeno, mentre la quasi totalità degli ambienti non saranno adeguati alla proliferazione clostridica e quindi la sopravvivenza di questi è legata a una presenza sotto forma di spora, forma di sopravvivenza del batterio metabolicamente inattiva.
Tramite queste spore può avvenire la contaminazione: la maggior parte delle volte da ciò non origina nessuna infezione o colonizzazione perché non presenteremo al clostridio un ambiente adatto per la proliferazione, ma può capitare che si creino, nell’organismo, delle zone di microaerofilia o anaerobiosi (per esempio zone ischemiche che possono presentarsi in seguito a traumi dove non c’è più vascolarizzazione) e dunque diventano zone adatte per essere colonizzate. Perciò il metabolismo fermentativo di questi batteri è attivo solo in condizioni estremamente riducenti perché, essendo anaerobi obbligati, non sono in grado di utilizzare l’ossigeno come donatore di elettroni.
Habitat
• Ambiente ubiquitario: suolo, scarichi fognari, ambienti acquatici con elevato contenuto organico.
• Organismi: colonizzazione apatogena da parte di una serie di clostridi, compresi quelli patogeni per l’uomo, dell’intestino dei mammiferi, un microambiente anaerobio dove si creano zone di importantissima fermentazione da parte delle flore commensali e residenti.
Si generano così un ambiente riducente idoneo e una condizione di anaerobiosi adatta alla proliferazione dei clostridi. In particolare questi batteri vanno a colonizzare gli intestini dei ruminanti.
La proliferazione dei clostridi porta alla generazione di numerose spore le quali spargendosi nell’ambiente circostante possono portare alla sua contaminazione. Vengono a crearsi così ambienti fortemente a rischio di contaminazione, come ambienti rurali, ippodromi, stalle, maneggi, ecc.
Le spore di questi batteri sono resistenti a
• Disinfettanti chimici
• Esposizione ai raggi ultravioletti
• Temperature di ebollizione per un certo periodo di tempo
Sono distrutte solo da un processo standard di autoclavaggio (121° C per 15 minuti)
Sporulazione
La spora si genera quando il batterio fa sensing delle condizioni avverse (ovvero la presenza di ossigeno). Questo innesca un processo di regolazione genica che coinvolge 200/300 geni portando alla generazione di una cellula figlia anomala, non risultante quindi da una scissione binaria, diversa dalla madre, la quale morirà dopo aver dato alla figlia le caratteristiche che la rendono inerte e resistente.
Verranno generate una serie di strutture resistenti di protezione, all’interno delle quali ci sarà un contenuto disidratato, che contiene enzimi inattivi e l’acido nucleico. Al momento opportuno la spora (che è l’equivalente del seme nelle piante) dovrà germinare dando origine a un nuovo batterio con un acido nucleico integro e degli enzimi che faranno ripartire il metabolismo e che porteranno alla rottura degli strati coriacei, i quali rendono la spora resistente a una serie di aggressioni ambientali.
Potere patogeno
Il potere patogeno di tutti i clostridi di interesse medico risiede, oltre che nella loro resistenza estrema a livello ambientale, anche nella produzione di tossine, che danno intossicazioni più o meno importanti nella condizione di germinazione, ovvero quando il batterio si troverà in condizioni ottimali per poter proliferare.
Nella maggior parte dei casi l’uomo viene intossicato non direttamente dal batterio, ma dal prodotto tossico acquisito come precostituito da situazioni in cui il batterio ha potuto proliferare e dare origine ai suoi prodotti patogeni.
I due ceppi batterici più canonicamente associati a malattia sono il clostridium botulinum, agente eziologico del botulismo e il clostridium tetani, agente eziologico del tetano. Entrambe sono malattie mortali mediate dalla produzione di due esotossine che sono rispettivamente la tossina botulinica e la tossina tetanica. Per quanto riguarda il clostridium tetani vi è l’obbligatorietà del vaccino nei primi mesi di vita perché esso è estremamente diffuso nell’ambiente ed è facilissimo acquisirlo, a differenza del botulismo che è più raro.
Le tossine prodotte dai clostridi sono tutte delle tossine binarie A-B toxin, nelle quali una regione della tossina è deputata al binding del recettore (B), mentre la seconda è la vera zona attiva della tossina (A). La tossina entra nelle cellule bersaglio che identifica attraverso la regione di binding e poi rilascerà all’interno il frammento attivo (active site) che andrà ad interagire con differenti bersagli a seconda del tipo di tossina.
Clostridium Perfrigens
È un batterio capsulato, Gram positivo, ubiquitario componente della flora del tratto gastroenterico e qualche volta anche della flora vaginale. È un patogeno importante perché, come tutti i clostridi, produce esotossine che possono raggiungere anche zone lontane dal sito d’infezione, ma è l’unico di questa famiglia che agisce come patogeno anche producendo enzimi degradativi (o istiolitici, o idrolitici) che gli garantiscono un forte potere invasivo, indipendentemente dall’azione delle esotossine.
Ha molti fattori di virulenza e produce numerose tossine tra le quali la fosfolipasi C, che rompe le membrane cellulari, uccidendo le cellule che entrano in contatto con essa, e ha un’attività necrotizzante a livello tissutale, divenendo dunque un fattore determinante nell’insorgenza della gangrena gassosa ( o mionecrosi tissutale indotta dei tessuti profondi).
La necrosi tissutale favorisce un’ulteriore proliferazione di questo batterio anaerobio. Un’altra importante tossina è la tetatossina, che è un’emolisina; vi sono poi ialuronidasi, proteasi, collagenasi e tossine citolitiche che gli conferiscono un alto potere di invasività tissutale . Produce anche un’enterotossina molto aggressiva che va ad alterare la permeabilità della membrana dell’ileo e del cieco e ha una funzione infiammatoria importante, degradando le funzioni dell’enterocita.
Patogenesi
Causa celluliti e fasciti (riscontrabili anche per gli Stafilococchi e gli Streptococchi) e porta, nella sua versione di maggior capacità di aggredire, a una malattia detta gangrena gassosa o mionecrosi tissutale indotta dei tessuti profondi, in genere in seguito a ferite gravi come ferite da guerra o ferite traumatiche da schiacciamento (in esse si creano zone ischemiche di anaerobiosi dove il batterio può replicarsi).
Si chiama gangrena gassosa perché in condizioni ottimali questo batterio ha un’elevata attività replicativa, un tumultuoso metabolismo, che produce come risultante della fermentazione una grande quantità di gas che si accumula in bolle e produce crepitii. L’unico modo per eradicare la problematica è amputare o asportare la zona colpita, per evitare che l’infezione vada sempre più a coinvolgere una maggiore quantità di tessuti.
Può causare anche un’endometrite necrotizzante, perché facendo parte anche della flora vaginale, in condizioni di aborto, può succedere che la flora vaginale stessa, contenente questo clostridio, vada ad infettare tessuti necrotici che si formano in seguito all’aborto (anche spontaneo) . Un’altra malattia abbastanza caratteristica è dovuta alla presenza del batterio nel tratto intestinale, che causa un’intossicazione alimentare, se la tossina è assunta dall’esterno o un’enterite necrotizzante, se il batterio colonizza l’intestino e replicando produce enterotossine all’interno dell’organismo.
Trattamento
Le infezioni da clostridium botulinum e clostridium tetani sono replicazione-indipendente, ossia non serve la replicazione del batterio per dare malattia, ma l’unico fattore di virulenza è la tossina, quindi la terapia antibiotica non avrebbe alcun effetto. Laddove, invece, parte della patogenesi è la replicazione del batterio è invece importante effettuare una terapia antibiotica e in genere il clostridium perfrigens è sensibile alla penicillina.
L’altra terapia importante (anche di prevenzione) è la camera iperbarica, che da un’iperossigenazione tissutale esogena che favorisce il rallentamento metabolico della proliferazione del Perfrigens e il mantenimento in vita dei tessuti colpiti, dove possibile. Questo trattamento, associato alla terapia antibiotica, limita la progressione della malattia. Il Clostridium Perfrigens, come il botulismo, è piuttosto raro.
Clostridium Botulinum
Caratteristiche
È un anaerobio strettissimo che produce delle neurotossine che portano a una paralisi. Il clostridium botulinum si prende dall’ambiente che è stato contaminato da feci degli intestini dei ruminanti; le spore si depositano sulle piante oppure sono presenti, oltre che negli intestini, anche nei tessuti degli animali e, dunque, le assumiamo mangiando verdura o carne. Un esempio di alimento, dal quale possiamo contrarre il clostridium botulinum, è la conserva di pomodoro messa in aerobiosi, nella quale il batterio può proliferare, ma non è questa la fase in cui vengono prodotte le tossine. Le tossine vengono generalmente prodotte nella fase pre-sporigena, e dunque, nell’esempio precedente, nel momento in cui si espone la conserva all’aria. Il batterio, avvertendo la presenza di ossigeno, prima di divenire spora, libera tossine .
Patogenesi
A oggi la tossina botulinica è il veleno naturale più potente che conosciamo (250mg basterebbero per sterminare l’intera popolazione mondiale).
Questa tossina va a bersagliare le placche neuromuscolari. In genere in esse, il motoneurone eccitatorio rilascia il neurotrasmettitore eccitatorio (es. acetilcolina) attraverso le vescicole contraendo le fibre muscolari, in seguito il motoneurone inibitorio attraverso il neurotrasmettitore inibitorio (es. GABA) fa rilasciare il muscolo.
La tossina botulinica inibisce specificamente il rilascio dell’acetilcolina da parte delle vesciche presinaptiche, di conseguenza si avrà una paralisi flaccida, in quanto le fibre muscolari non si contrarranno più, a volte definitivamente. La tossina botulinica viene utilizzata anche per ridurre le rughe, ma il suo utilizzo può limitare la mimica facciale.
L’effetto di tale tossina è estremamente duraturo. Se non si riesce a contenere la diffusione sistemica di questa tossina, soprattutto nella porzione superiore dell’organismo, si arriva alla morte per blocco del diaframma e del muscolo cardiaco (colpisce dunque sia muscoli volontari che involontari).
La tossina botulinica è costituta da 8 isoforme (A,B,C-α,C-β,D,E,F,G) che agiscono sul sistema vescicolare, bersagliando momenti diversi della secrezione
• Le isoforme B,D,F e G tagliano la sinaptobrevina
• Le isoforme C tagliano la sintaxina e la proteina SNAP-25
• Le isoforme A ed E tagliano la proteina SNAP-25 e impediscono il rilascio di acetilcolina, andando ad agire su molecole coinvolte nella fusione della vescicola acetilcolinica a livello della terminazione nervosa
Classificazione
Esistono 3 tipi di botulismo
• Botulismo “classico”: spiegato in precedenza
• Botulismo infantile: se le spore raggiungono un intestino in cui non c’è ancora una flora residente consistente, possono germinare e dare una tossinfezione intestinale, che spesso è autolimitante e causa gravi problemi intestinali. Quasi mai la tossina entra in circolo causando una malattia sistemica.
• Botulismo da ferita (raro): molto simile al tetano da ferita
Trattamento
Il vaccino è difficile da ottenere e possiamo contenere il botulismo in modo soddisfacente anche semplicemente con la prevenzione.
È importante non dare il miele a bambini di età inferiore a un anno per evitare il botulismo infantile
Clostridium Tetani
È un clostridio strettamente anaerobio, che in coltura non riusciamo a vedere come bastoncello, ma come “bacchetta di tamburo” perché è talmente anaerobio, che è sempre in condizione di sporulare.
Patogenesi
La patogenesi del tetano è legata alla singola tossina tetanica, perché la malattia causata dall’infezione di una ferita è la forma più comune e viene definita tetano da ferita. Ogni volta che infettiamo una ferita con le spore tetaniche siamo ad altissimo rischio di contrarre il tetano (evento invece raro per il Clostridium botulinum) e se non controllassimo la malattia col vaccino sarebbe estremamente diffusa.
È facile infettarsi con le spore del tetano venendo a contatto col ferro arrugginito, che rilascia schegge causando una ferita lacero-contusa dove si crea un microambiente di necrosi tissutale all’interno del quale il batterio può replicare. Quando si sospetta una contaminazione si consiglia di incidere la zona lesa e far sanguinare per ossigenare il tessuto e impedire una progressione della malattia.
Essendo il batterio strettamente anaerobio in vivo tenderà quasi immediatamente a sporulare, producendo prima le due tossine
• Una tetanolisina, che non causa nessun danno a livello dei tessuti
• La tetanospasmina, l’unico vero fattore di virulenza del clostridium tetani
Questa è una tossina A-B e la sua zona attiva è una proteasi che taglia la sinaptobrevina, agendo a livello muscolare come nel botulismo. La binding side della tetanospasmina, però, trova il proprio recettore non sul motoneurone eccitatorio (come avviene nel botulismo), ma sul motoneurone inibitorio, che non secernerà il neurotrasmettitore inibitorio (GABA o glicina). Questo porterà alla contrazione tetanica, un’ipercontrazione muscolare detta spasmo tetanico del muscolo, che non riesce a rilassarsi.
Il risultato è una paralisi spastica (non flaccida come nel botulismo) che, nelle fasi terminali, porta a contrazione dei muscoli dorsali, con conseguente inarcamento della schiena, mentre uno dei primi segni è il risus sardonicus, contrazione dei muscoli facciali che porta a questa espressione simile a un sorriso.
Quando la tossina si diffonde, la malattia si definisce tetano generalizzato.
Quando invece veniamo a contatto con una quantità minima di spore il tetano può essere definito localizzato, in quanto la tossina che verrà prodotta riuscirà ad agire solo a livello del muscolo locale e non arriverà al circolo diffondendosi a tutto l’organismo. Il tetano localizzato in genere precede quello generalizzato, quindi un’anamnesi attenta dovrebbe prevenirlo
.
Molto frequente è il tetano neonatale, diffuso nei paesi a basso livello di sviluppo, dove si hanno parti in condizioni igieniche scarse e dove si può avere infezione del cordone ombelicale, che deve andare in necrosi per creare il moncone, determinando una regione ad altissimo rischio di tetano. La mortalità è molto alta.
Trattamento
Il vaccino per il tetano è uno dei vaccini più vecchi che usiamo, ad ampia diffusione. È molto sicuro ed è basato sulla capacità che il nostro organismo ha di generare anticorpi che vanno ad inibire in maniera definitiva l’eventuale presenza di tossina nell’organismo.
La tossina del tetano è una proteina fortemente immunogenica, che resta tale anche se vengono modificati i suoi siti attivi con trattamenti chimici, che ne cambiano la conformazione rendendoli inattivi, ma mantengono inalterate le regioni immunogeniche.
La tossina così modificata si chiama anatossina o tossoide e può essere iniettata nel soggetto, dove darà origine a una reazione che produrrà anticorpi neutralizzanti, i quali saranno in grado al momento della presenza della vera tossina nell’organismo di andare ad impedire gli effetti deleteri che questa può produrre. La vaccinazione è obbligatoria a livello infantile (al terzo mese di vita) ed è fortemente consigliato effettuare i richiami successivi per mantenere il numero degli anticorpi sopra un certo livello.
Terapia
Nei pazienti sopra ai 60 anni l’incidenza aumenta drasticamente, in parte perché allora non era diffuso il vaccino, ma soprattutto perché l’immunità acquisita in età infantile, senza mai richiamare il vaccino, a un certo punto si perde.
In caso non si fosse coperti da vaccinazione, ai primi sintomi (spesso si tratta di tetano localizzato) è possibile andare a trattare con anticorpi preformati, che vanno a neutralizzare la tossina. Questi anticorpi si possono somministrare in loco per via intramuscolo, da dove entrano in circolo.
Di solito si tratta di sieri iperimmuni di soggetti vaccinati di recente. Questi soggetti producono una grande quantità di anticorpi, che vengono prelevati con il siero e vengono purificate da esso le immunoglobuline contro la toscentrosina tetanica che si iniettano nei soggetti che non sono stati sottoposti a vaccinazione. Tali sieri devono essere comunque utilizzati con cautela in quanto emoderivati.
Si attua dunque un’immunoprofilassi passiva quando c’è il rischio elevato di contrarre malattia o un’immunoterapia passiva quando già è presente il tetano e questa terapia serve a prevenirne l’evoluzione. Gli antibiotici non hanno nessun effetto sulla tossina tetanica, sono solo in grado di far sporulare il batterio (reazione inutile o addirittura dannosa).
Fonti/Sources
msdmanuals botulismo
msdmanuals tetano
msdmanuals perfrigens
epicentro botulismo
epicentro tetano
Immagini/Pictures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
Please join us on discord.
At work, anaerobes are their own bench that require special chambers and dedicated microbiologists to stay there the whole shift.
But, the work ups and stuff aren’t that much different. Just more names to remember.
The big difference I imagine is in the equipment of the laboratory that must be specific to work in the absence of air, and in the cost that this technology has .
Yes, the media have to be in anaerobic condition first. And all work is done in an anaerobic chamber that has the gas tanks changed every so often.
I actually have no idea of the cost, but you can have small boxes with gas packs to gloveless chambers that are in 5-digits.
It’s not super expensive, just lots of upkeep.
Congratulations @riccc96! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPTo support your work, I also upvoted your post!
This post was selected, voted and shared by the discovery-it curation team in collaboration with the C-Squared Curation Collective. You can use the #Discovery-it tag to make your posts easy to find in the eyes of the curator. We also encourage you to vote @c-squared as a witness to support this project.
Wow! This laborious post needs to be read by medical experts my friend and I doubt that the ordinary steemians, such as myself will make heads or tail of the medical language.
However it is a very impressive post that will be sure hopefully to illicit professional responses.
Blessings!
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.
articolo interessantissimo....cancrena alla gamba che va amputata....io mi batto per un'ottima qualità della vita anche senza un arto e che non si soffra nel rimuoverlo!!!