Ovarian Cancer - The Silent Killer | A Deep Analysis
Ovarian Cancer, also known as "The silent killer" is 4th most common cancer in women. The first three are Breast, colon, and lung respectively. Ovarian cancer contributes to 16- 19 % of the genital cancers and also the most common cause of death in the US after breast cancer. But this is less active in Asian countries like India and Japan. In the US, 1 in 70 women might develop ovarian cancer.
Credits, Pixabay(Under resuse license)
Epidemiology and Risk Factors
The highest number of cases is recorded in developed countries like USA, UK, Sweden. The incidence per 100,000 is given below.
- Sweden - 14.9
- Norway - 14.2
- USA - 13
There are various risk factors that lead to ovarian cancer. Some of them are discussed below.
- Nulliparous women are more likely to develop ovarian cancer.
- Repeated trauma to the ovary (Epithelial lining) promotes carcinogenesis.
- Frequent use of Ovulation Inducing drugs.
- History of cancer in the family.
- History of other gynecological cancers like cervical cancer, endometrial cancer.
The relation between Genetics and Ovarian cancer.
We can observe hereditary ovarian cancer in toe different types. Hereditary breast-ovarian cancer syndrome and Hereditary nonpolyposis colorectal cancer.
Hereditary breast-ovarian cancer syndrome (BOC) -This form is seen in 90% of the hereditary ovarian cancers. The main gene mutations are BRCA1 and BRCA2. Presenting patients are of young age.
Hereditary nonpolyposis colorectal cancer (HNPCC) - Also known as Lynch II syndrome is an autosomal dominant disorder. Women with this syndrome have a risk of developing endometrial and ovarian cancer. This occurs due to mutations in DNA repair genes (MLH1, MLH2, MLH3)
Types of Ovarian Cancers
Most of the malignant ovarian tumors are of epithelial origin. This constitutes about 92% of all ovarian cancers. The other tumors like germ cell tumor, sex cord tumor are very rare and will be described in my upcoming article. For now, we will be discussing Malignant Epithelial cancer only.
Epithelial Cancer of Ovary
This is the most common ovarian cancer constituting more than 90% of all ovarian cancers. Also in 50% of cases it is found to be bilateral. Epithelial origin is further divided into cystic and solid type. Cystic type is found to be more common than solid.
Cystic Type - With a naked eye view, the tumor looks shaggy, with papillary (finger-like) projections at many places. The cut section shows areas of hemorrhage and might be filled with gelatinous fluid.
Solid Type - Unlike cystic type, this tumor appears to be smooth and lobulated. Sometimes blood vessels are also seen. The cut section shows granular brain-like appearance and areas of necrosis.
Does this Cancer spread to other Parts?
Well, the answer is yes, but only in later stages of cancer. We will discuss the stages later in this article.
The natural path of spread is along the peritoneal surface which involves intestinal, parietal, under the diaphragm, etc. But Modes of spread are
- Trancscelomic
- Lymphatic spread
- Direct Spread
- Hematogenous Spread
Transcelomic Spread - The cells from the tumor are found to be floating in the peritoneal fluid which later gets deposited in the different parts of the genital region.
Lymphatic spread- The lymphatic spread to other parts is mostly by paraaortic and superior gastric nodes. Also, Supraclavicular nodes (Virchow's nodes) are enlarged due to the blockage of the thoracic duct because of a tumor cell collection.
hematogenous- through the bloodstream to bones, lungs, liver, and brain.
The Stages of Ovarian Cancer
| Stages | Events |
|---|---|
| Stage 1 | Tumor is limited to Ovaries |
| Stage 1a | Tumor is limited to one ovary, with no ascites. |
| Stage 1b | Tumor is limited to both ovary, with no ascites. |
| Stage 1c | Tumor is limited to one or both ovary, with ascites. |
| Stage 2 | Tumor in one or both ovary, with pelvic extenson. |
| Stage 2a | There is impants of the tumor to the uterus or fallopian tubes, no ascites. |
| Stage 2b | There is impants of the tumor to other tissues, no ascites. |
| Stage 2c | both 2a and 2b, with ascites. |
| Stage 3 | one or both ovaries with peritoneal implants outside the pelvis with lymph nodes. |
| Stage 3a | Grossly limited to pelvis. |
| Stage 3b | peritoneal metastasis, beyond pelvis < 2cm |
| Stage 3c | peritoneal metastasis, beyond pelvis > 2cm |
| Stage 4 | Distant metastatis which might include liver. |
Here stages I and II are less severe but Stage III and IV are very severe and malignant.
Some Clinical Feature of Patients
Profile of the patient: 60% of the women are post-menopausal and 20% are premenopausal. But it should be noted that no age group is immune to ovarian cancer. Also, there might be a history of nulliparity and family history.
Symptoms ( Patient complaints):
In early stages, this cancer is silent or asymptomatic. The presenting complaints to the doctor are not specific at all. Those symptoms can be as follows:
- distention of abdomen and discomfort.
- severe flatulence and pelvic pain.
- Loss of appetite and sense of bloating.
- dull aching pain.
- small enlargement might be seen.
Later stages might show these symptoms:
- Rapid abdominal swelling.
- Sudden pain in the abdomen.
- sudden and rapid weight loss.
- Respiratory distress
- Abnormal mensturation.
Signs ( what Doctor observes):
with a basic general examination by the doctor, these signs are seen.
- wasting of the body mass and pallor.
- Late cases might show jaundice.
- Left supraclavicular gland swelling as explained above.
- Edema of legs due to lymphatics obstruction.
- The liver is enlarged and firm
- Mass can be felt on unilateral or bilateral sides.

Fig: Signs of ovarian cancer showing enlarged left supraclavicular node. ( Credits: Picture belongs to me @idoctor)
Special Investigations Performed by the Doctor
The cytological examination is done to detect the malignant cells. This process is done after the collection of fluid from the abdominal cavity. This process of collection of fluid is known as "cul-de-sac" aspiration.
The tumors marker cells are observed. In epithelial type, a specific tumor marker is not found but CA-125 level > 65 U/ml is very suggestive. These two processes are performed to confirm malignancy.
Other investigations to observe the extent of malignancy.
- Chest Xray: To see the lesion in the lungs.
- Barium Enema: to see the lesion in the colon.
- ultrasound imaging
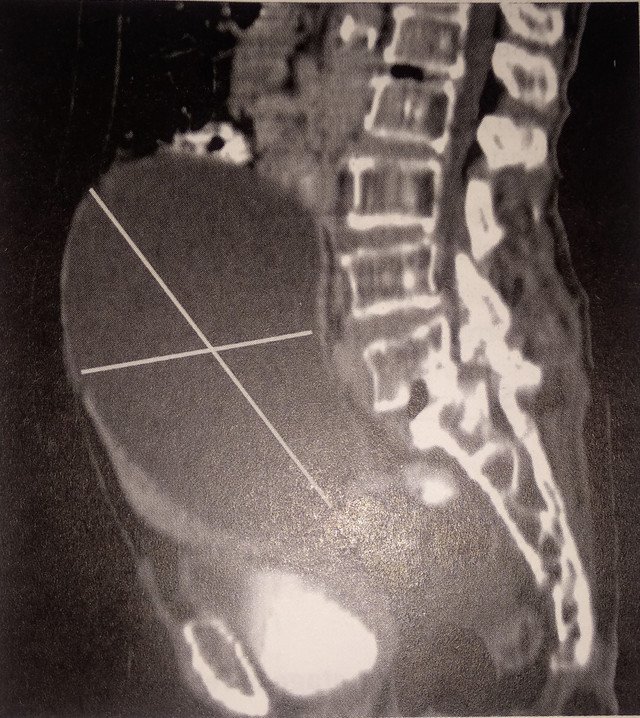
- Computed tomography (CT scan): This is very helpful for the assessment of lymphatic spread, metastasis, and also helps in the staging of ovarian cancer.
- Magnetic Resonance Imaging (MRI): It is very similar to the CT scan and It determines the nature of the ovarian tumor.
- Examination under anesthesia
- Uterine curettage.
How is the Diagnosis Made?
In the early stages, it's very difficult is to diagnose ovarian cancer hence the term "The Silent Killer". Most of the time it is very late until it is diagnosed. The reasons for bad prognosis are as given below:
- There is no specific age for Ovarian cancer.
- The symptoms are mostly asymptomatic. Even though symptoms exist, they might be not specific to ovarian cancer.
- The tumor is not related to its size. Big tumors may be benign and small tumors may be malignant.
Because of these reasons, at the time of diagnosis, about 75% of the patients have metastases beyond the pelvis. The most common locations for metastasis are peritoneum, another ovary, liver, lungs, and uterus.
Detection of malignant cells in Ascitic fluid: As mentions above in the Investigation part.
operative findings: This is found accidentally while performing surgery for other reasons. Mostly, peritoneum fluid is hemorrhagic which is suggestive of malignancy. The tumor might be seen directly while performing surgery or nodules on the peritoneal surface is seen.
Histological finding: This is done after a biopsy from the suspected tumor. This confirms this malignancy and also identifies the nature and grade of the tumor.
How do we manage this cancer?
It's very difficult to diagnose this cancer. So, various screening procedures are performed for high-risk women. The criteria for a woman to be in the high-risk category follow:
- Age of more than 60
- Family history of cancers like breast, cervix, endometrial.
- history of benign tumors like ovary and breast
- Family history of BRCA1 and BRCA2 gene mutation
- woman with no pregnancy till menopause
- late menopause
- Infertility
- BMI > 30
- Women working in asbestos industries.
Basic Screening Procedures
Periodic Clinical Examination: In High-risk women a periodic clinical examination is performed. which consists of bimanual pelvic examination and vaginal examination to detect a mass.
Detection of tumor markers: CA-125 is the tumor marker which is widely used for the screening of ovarian cancer. But it's not a tumor-specific marker. CA-125 can be raised in the following conditions too.
- Normal woman
- other cancers like breast, colon, lungs
- pelvic inflammatory disease (PID).
Also, the level of CA-125 falls after the surgical removal of the tumor or after successful chemotherapy. Another marker HE-4 can also be found in a woman with ovarian cancer. Therefore detection of both CA-12 and HE-4 is highly suggestive of malignancies.
Treatment of Ovarian Cancer.
There are various ways to treat ovarian cancers. They might be used in combination or alone. The various ways are surgery, Chemotherapy, Radiotherapy, and combination therapy.
Surgical treatment: This is the mainstay treatment of ovarian malignancies. The aim is to stage the tumor to decide the therapy or to completely remove the tumor.
Things did while performing surgery.
- A vertical incision is made to minimize the chances of the rupture of tumor.
- Better exploration is done.
- The character of the peritoneal fluid is noted.
- A systemic manual exploration is done which consists of palpation of liver, diaphragm, lymph nodes in a clockwise way starting from the cecum.
- pelvic parts are explored.
- Any kind of metastatic deposits is noted under the surface of diaphragm and peritoneum.
- Multiple biopsies are taken.
Whats type of surgeries are performed?
In the early stages of diseases (Stage I): Unlilaterla oophorectomy ( Removal of an ovary) is done to preserve fertility. In an elderly woman Hysterectomy (Removal of the uterus) is done with Bilateral salpingo-oophorectomy (removal of fallopian tubes and ovaries)
In Later or advanced stages: Debulking surgery is done, which includes total hysterectomy( removal of uterus totally), bilateral salpingo-oophorectomy, omentectomy( removal of omentum), removal of lymph nodes.
Chemotherapy:
In early stages like Stage I, no chemotherapy is needed. In all other stages of cancer, chemotherapy with carboplatin and paclitaxel is given. Platinum-based compounds (cisplatin and carboplatin) are very effective in therapy.
Indications for Chemotherapy: Imaging shows a very advanced ovarian cancer or the patient is incompetent for surgery.
Radiotherapy: It means providing a high dose of radiation to the cancer cells, which in turn damages the DNA, and hence cells cannot multiply. But this therapy is minimally used in this cancer because it has a very little scope. Chemotherapy and surgery are preferred over radiotherapy.
What are the reasons for poor outcomes in ovarian cancer?
- it's almost diagnosed late every time.
- There is no pre-invasive stage of the disease that can be detected.
- Screening procedures are not specific.
- There is no relation between tumor size and symptoms.
- the tumor is freely mobile.
You stayed until the end. Thank you so much for reading guys hope you enjoyed it.
References:
[1] https://www.mayoclinic.org/diseases-conditions/ovarian-cancer/symptoms-causes/syc-20375941
[2] https://www.healthline.com/health/cancer/ovarian-cancer-early-signs
[3] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6500433/
[4] https://www.cancer.org/cancer/ovarian-cancer/treating.html
*All the images used are copy-right free*
@tipu curate
Upvoted 👌 (Mana: 8/12)
Very informative. I have a question . how does ovarian cancer cause ascites?
Thanks :) .. I forgot to answer this in my article. Actually, the ovarian mass blocks the peritoneal fluid outflow through the diaphragm. Also, there is increased transduction of serum across the peritoneal lining which leads to ascites.
Gracias por compartir tan interesante contenido en el campo de la medicina y la suma importancia que debe tener conocimiento sobre este tipo de cancer.
Glad you liked it :)
Hey @idoctor,
very interesting overview about ovarian cancer.
I would like to upvote them but I have no idea whether the images you use are copyright-free?
Would you please be so kind to tell us if there are potential copy-right issues???
Thank and regards
Chapper
Thank you for your concern. Actually, not all of them are copy-right free. but I have mentioned the appropriate sources under the respective pictures. If this is an issue, please tell me. I will remove those pictures and use my own.
For stemsocial upvotes it is important that no copy-right issues occur in supported posts.
Please substitute the images if you want to receive stemsocial support.
Regards
Chapper
Thanks, I just updated my article and used my own pictures. All of them are copyright free.
Concerning the table: You did the image but the content is from a source that probably is copyright-restricted. Would you please create an own table?
Thanks
Sure, made my own table.
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider supporting our funding proposal, approving our witness (@stem.witness) or delegating to the @steemstem account (for some ROI).
Please consider using the STEMsocial app app and including @stemsocial as a beneficiary to get a stronger support.