SARS-CoV-2: Repositivization, pathogenetic mechanism, therapies.

Public domain - Source
What is the current knowledge about the virus that has shocked the whole world?
What do the clinical evidence and studies that are being conducted globally tell us?
There are still many doubts, but researchers and doctors who face Covid-19 every day begin to clarify some points.
Repositivization, antibody duration, immunity
We are attending these days to events such as the repositivization of patients who had recovered after the disease and had tested negative at 2-3 and sometimes even 4 consecutive swabs.
Recently, an important study published in Nature Medicine has highlighted the presence of antibodies in all patients who have had the disease.
But what kind of antibodies are they?
The same questions are asked in Atlanta and Korea. To date, the nasopharyngeal swab is used as the main reference, which is then analyzed by CRP (C-reactive Protein) and the serological ELISA with recombinant S1 (spike) protein with final enzyme reaction is used as a test for the confirmation of antibodies.
Today there is a problem of false positives, because the tests currently used also "see" similar antibodies, or there are false negatives because the antigen on which the test is structured is not well exposed and therefore is not captured by the antibodies.
Once a positivity to the test is highlighted, this does not guarantee protection from re-infection and if there is even minimal protection, it's not known if this can be effective compared to the possible evolution of the disease in a more serious form.
The researchers are also wondering which title to look at while thinking about a possible protection: IgG, IgA, these aspects are still very nebulous.
It's very probable that immunity is forming but it is very difficult to understand if this immunity is linked to the disease or infection.
For the virological test, replication is a very sensitive process, because in theory even a single copy of the virus can be amplified to have a positivity after 35-40 CRP cycles.
You then enter a twilight zone, especially if you give a positive result on a negative one without a quantification (but only in qualitative measure).
There are those who become positive after only 3 amplification cycles, so that person has hundreds of thousands of copies of viral RNA. But it's possible, at the same time, that a person has CRP with a positive signal after 30-35 amplification cycles.
It must be considered that positivity can also develop by amplifying dead viral material, pieces of the virus and therefore this material is not infectious. So we must consider that not all positive CRP are identical, they are outcomes to be interpreted differently.
For this reason, many hospitals and centers are moving towards traditional serology, based on the isolation of the virus in culture, with the possibility of effectively separating the antigen if there is truly the viral presence and not only its fragments.
Also because there are some specialized cells of the respiratory system, such as ciliates, secretory that have a very slow turnover and therefore, if they are even minimally infected with the virus, they go into apoptosis and remain in the mucous membrane for a long period.
In this way they can be identified by the swab, detecting a positivity.
This is a very important aspect, given that today we have people with a positive outcome even after 60 days who are not taken out of isolation for the supposed infectious risk.
In these cases, it's evident whether the virus is really present and infectious by combining the diagnostic techniques in use, checking whether the subjects have developed neutralizing antibodies and putting them in culture.
People who contract Coronavirus infection, asymptomatic aside, are infectious from two days before the appearance of the first symptoms up to 7 days after the presentation of the same.
Disease phases and pathogenetic mechanism
Something more has been understood about pathogenetic mechanisms and three disease phases have been defined for which it will probably be necessary to use three different types of therapies:
- viremic phase
- pulmonary phase
- inflammatory phase
The main points to date are these.
In general, this virus comes into contact with the human body from the nasal area.
The microorganism is a coronavirus with a fairly classical structure, with a single positive chain RNA that quickly translates into proteins.
On the surface there is a protein, the S, which is formed of two subunits, S1 and S2.
The S1 subunit binds to ACE2 which is the analogue of ACE which is normally inhibited to decrease the production of angiotensin 2 thus activating the mechanisms that increase blood pressure.
ACE2 is a very interesting molecule; it's expressed in the respiratory system at various levels and also in the second type pneumocytes, therefore those that act as alveolar surfactant.
It's still under discussion how much it actually circulates more deeply than other viruses, such as plasma concentration. The viremic phase is probably very short and therefore difficult to capture clinically.
When the virus binds to ACE2, then direct damage begins due to local inflammation mechanisms. ACE2 is a molecule with anti-inflammatory activity both in the lung and in the endothelium and in other tissues, its expression is induced by interferon and therefore it is possible that there is a response to interferon that may initially favor the spread of the local virus in the respiratory system.
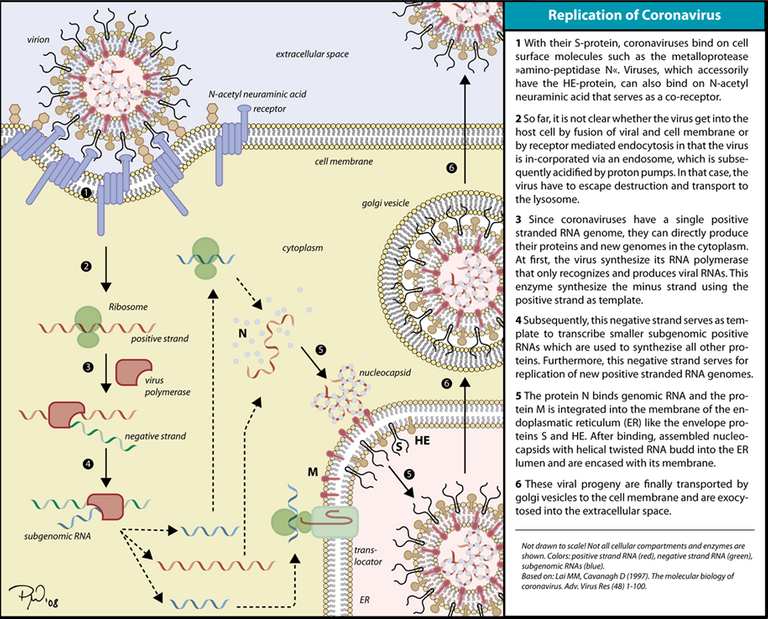
Image CC BY-SA 3.0 - Source
{kind=link}
Then, an initial respiratory disease arises, which then becomes lung disease, the complex evolution of which has been identified as interstitial pneumonia.
It must be said, however, that the analysis of 11 autopsies in Atlanta, obviously of the most serious cases, revealed serious thrombophilic microvascular damage spread far more impacting on the patient than interstitial pneumonia with accumulation of neutrophils. The 50 autopsies analyzed in Italy, between Sacco Hospital in Milan and Bergamo Hospitals, also gave similar results.
Hence, much is being discussed about the origin of this interstitial pneumonia to understand if it is primarily of alveolar origin or if it is primarily of a vascular type.
However, there is always a severe final phase of the disease that leads to death, in which there is a whole series of alterations of inflammatory homeostasis, mainly coagulation.
There appears to be a systemic situation disproportionate to viral replication that doesn't seem to be so high. It almost seems like an intravascular coagulation disseminated without bleeding even with very low or absent viraemia and this is still a mystery that is being sought to be clarified.
Among the many factors investigated, Interleukin 6 (IL-6) seems to have an important role.
The main function of ACE2 is to take angiotensin 2, which is a peptide of 8 amino acid residues, cut out the last one of these 8 and thus create a variant called angiotensin 1-7.
The latter, instead of binding to receptor 1 angiotensin, binds to receptor 2 angiotensin which has a whole range of anti-inflammatory effects.
If ACE2 is not present or not functional, an imbalance occurs whereby the production of angiotensin 2 by ACE1 creates a stimulation of angiotensin receptor 1, generating a strange molecule called ADAM17.
Structure of the ADAM17 protein - Image CC BY-SA 3.0 - Source
{kind=link}
This is a surface metalloprotease that does something that appears to be central to the pathogenesis of this disease, cuts the IL6 receptor that binds to circulating IL6 and amplifies the damage, becoming available for cells that normally do not have the receptor.
Possible therapies
The one mentioned above is a phenomenon described by immunologists for a few years and which seems to explain why molecules such as tocilizumab, which is a specific inhibitor of IL-6, or baricitinib which is a specific inhibitor of STAT-3 (the signaling IL-6 pathway) seem to have a particularly positive effect.
Another therapy that is proving successful and is being tested is the use of the plasma of patients recovered from Covid-19, who have undergone at least two negative swabs.
This therapy works, but care must be taken, because there may be, in addition to the antibodies, something more complex which inhibits the IL-6 amplified pathway. In fact, even doing plasma exchange without that of convalescents, it is seen effective in some patients.
For the first phase would seem suitable antivirals, since we are in the moment of virus replication.
Among antivirals, the one that seems to give the most promising results is remdesivir which should be used early, in the moderate-severe phase in which there is still a certain margin of recovery for the patient. Studies have shown about 1/3 decrease in mortality and reduced healing time.
This can also be a starting point for developing other antivirals, perhaps more powerful, and especially with the possibility of oral dosing, so that it can be taken more easily even at an early stage.
In contrast, remdesivir at a later stage, if the cytokine storm has already started, does not seem to be effective.
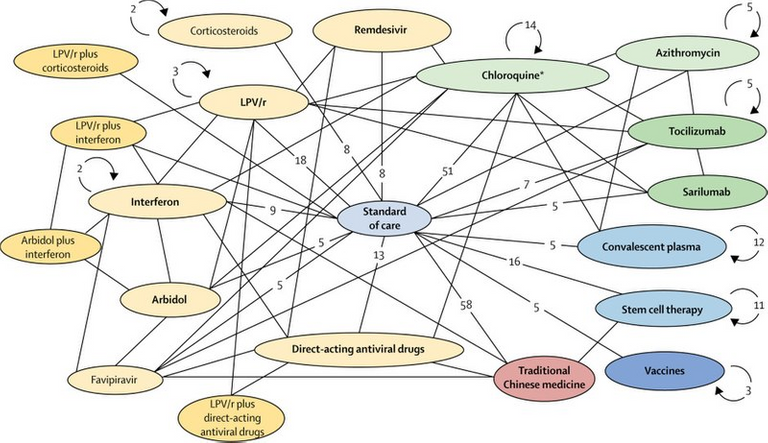
Image CC BY-SA 4.0 - Source
{kind=link}
The pulmonary phase requires a different approach and, as explained above, the anti-IL6 approach seems to work, even if there are no results from controlled studies on tocilizumab and, in some cases of use in the clinic, overinfections have been detected.
Chloroquine has shown little exciting results lately, so much so that in America its use is now not recommended, especially if associated with azithromycin, which would have led to fatal arrhythmias.
As for the mortality rate, today we cannot make comparisons between different countries, because only the final statistical data will give us a more precise result.
Probably, in some cases there has been an excess of mortality calculation and therefore we don't know how many deaths were actually due to the SARS-CoV-2 virus and how many to external pathologies treated late due to hospital overload.
It's clear that, when a system goes into overload, mortality explodes and this imbalance lasts a long time, making it more difficult especially to treat people with pre-existing diseases.
The experience of Italy has served many other states, including America, leading to an increase in hospital beds (in America they have tripled) and fewer health workers affected.
From a virological point of view, this seems a virus much more "vaccinable" than others as it does not integrate into the genome and therefore should not give latent infection.
We need to be more realistic about the timing of obtaining a vaccine, as it is certainly important to speed up the timing but always taking into account that, in addition to being effective, a vaccine can give negative side reactions such as ADE (antibody dependent enhancement), and other complications that they gave a worse immunogenic response.
The experience with the Dengue virus and the respiratory syncytial virus must make us think, these in fact gave completely anomalous answers.
I am confident that we will have a solution as soon as possible, but we must also know that a vaccine will have to be released only when there is assurance that it is effective against the virus and that any effects are absolutely not harmful at any therapeutic level.

Thanks to all of you for reading my article.
If you liked it, share it on your blog and write me a comment with your impressions.
See you soon!
GM
Sources
- https://www.pharmastar.it/news/covid19/covid-19-dai-test-ai-vaccini-passando-per-le-terapie-cosa-sappiamo-e-cosa-non-sappiamo-del-virus-che-ha-stravolto-il-mondo-32260
- https://www.nature.com/articles/s41591-020-0897-1
- https://ilritrattodellasalute.tiscali.it/notizie/articoli/coronavirus-colchicina-reumatologia-studio/
- https://www.scientificamerican.com/article/how-blood-from-coronavirus-survivors-might-save-lives/
- https://www.fondazioneveronesi.it/magazine/articoli/lesperto-risponde/dal-plasma-dei-guariti-una-possibile-cura-per-covid-19

Credits @doze
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider supporting our funding proposal, approving our witness (@stem.witness) or delegating to the @steemstem account (for some ROI).
Thanks for using the STEMsocial app and including @stemsocial as a beneficiary, which give you stronger support.
Thanks for the support 💪
Great post! Although this was super clear, I managed to have a few remarks and questions :)
Does that mean they move away from quick tests and go back to more accurate deeper and longer tests? At least my wife was moving her head agreeing with everything written in your post (she is working in hospitals, on the front).
Concerning the ACE2 issue, I don’t know whether you noticed this post. This is a very interesting piece of text that I warmly recommend.
Finally, I have two remarks concerning the last section: while the virus seems to be "vaccinable" as you said, if I am not mistaking, there is no proof we can get to herd immunity at all. Is this right? Finally, on different grounds, I am happy to see people to go away from chloroquine. Whilst I am not an expert, the trend of the latter was really way unscientific and made me feeling unsafe…
Thank you very much, I'm really glad you have appreciated my post!
I confirm, fully centered.
At the most critical moment, rapid tests had to be relied on because there was no time enough and all suspect cases had to be treated in the same way as certified ones. The aim was, of course, to keep the infections to a minimum, especially among family members.
Then, they realized that there were a number of false positives, due precisely to the presence of fragments of dead virus.
And now, with a little more calm, they are moving towards serology and virus isolation.
I'm glad your wife agrees, it's another important attestation.
About ACE2, I have read many things, but I have to say that the post by @scienceblocks (absolutely one of my favorite scientific authors), explains the dynamics in a really clear and precise way.
Herd immunity has never been considered in Italy as a possible solution. Virologists and epidemiologists have strongly contested those who fantasized about this solution, also because (I go to memory) we should have a percentage of around 95% of immune people...only a staunch supporter of no-vax theories can hypothesize such a thing at the moment.
We may approach when we have an effective vaccine...at that point, conspiracy theorists should be banned. 😁
Thanks for the clarifications!
If only they could be banned and never leave the pubs (where they should stay)... ;)
Happy Covid Party to everyone!! 🥂😄