The Year End Specimens I had to Deal with
So I got a laryngectomy, gastrectomy, radical prostatectomy and nephrectomy specimen all in within the last two weeks of the month. For some context, having even laryngectomy specimens is rare enough that I’m the second one on the department that gets to handled one after years of my seniors graduating. It’s an intimidating experience given the amount of preparation I had to do to review the larynx anatomy.
Even without the laryngectomy specimen, having those other specimens come meant I already took on assignments what my seniors never encountered in their years on duty. It’s like an alignment of the stars and feels like a sense of accomplishment but also getting crowned as the most toxic person on the department to always be the one receiving the complicated cases.

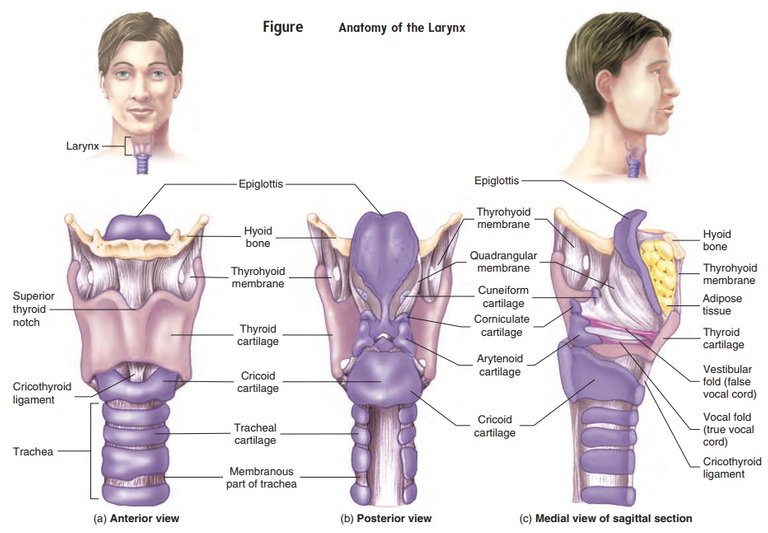
The anterior view where it still has the strap muscles intact (where the strings are attached). It's not a textbook image of the specimen so I had to read about the muscles too.

The posterior view of the larynx which now resembles what the textbooks would look like with a cut in between. Can you recognize some of the parts like epiglottis and tracheal regions from here? the center of the specimen you may even see the tumor peeking in between the narrow gap.
That’s my reputation alright and I actually asked for it. The more complicated cases I get the more I get good and I don’t want to graduate from the program and intimidated by rare cases.
We’re not the usual hospital that gets to receive these types of specimen but when we do, it had to be only one co-resident to consult with (not counting consultants). We could always ask for help but it’s also part of the training to troubleshoot at your level. Anyway, this came from an elderly where the cancer grew directly from the true vocal cords.

I use the sagittal section to bivalve it. The cream-tan to tan ill defined parts is the tumor invading the surrounding tissues. Hard not to miss. Remember, smoking is one of the risk factors for malignancies arising on these areas.
I immediately suspected this to be a case of squamous cell carcinoma just from the looks of it but of course I’ll be waiting for the slides to confirm. Even when it’s a different organ, having used to seeing, touching and feeling the texture of the tissue can already give you a clue on what you’re dealing with.
For extra measure, some printed pages from the book as a guide didn't hurt just to be sure I'm not going to get reprimanded for submitting the wrong sections.
I asked for help with the consultant on how to approach sectioning the specimen. The textbooks give you guide but these are just guides. Do I want to approach it as a sagittal section (vertical) or cross section (horizontal) and I got an answer that both could be used if I just want to demonstrate the depth of invasion of the tumor. Ok, it was slightly helpful advice. The textbooks would display the sagittal view to which I would go for in the end but having the cross section view was also viable too.
This is kinda alien speak but somehow without knowing how to approach sectioning you already get a meta insight on how you approach dissection even without the book’s guidance just by experience and troubleshooting.
The challenge for the specimen was trying to identify the smaller details of the normal anatomy but this proved to be futile considering the tumor already ruined the architecture. So I had to just cut where it’s supposed to be there.
I feel proud that I least get to handle this specimen for the first time. The odds are really slim that I’d see this again in a few years but with my rotten luck I might get another one or two before I graduate from the program. Even my consultants claim that handling such specimens were a rarity due to only few patients would opt for surgery given the poor prognosis and majority couldn’t afford chemo after so they just let palliative care do the work.
I haven’t even touched the subject of handling gastrectomy, radical prostatectomy and nephrectomy specimens yet which are their own lengthy story to tell for some other time.
If you made it this far reading, thank you for your time.
Posted with STEMGeeks