Colonic Tissue with Low Grade Adenocarcinoma
Below are some shots I took from a colonic tissue fragment from the sigmoid area from a 60 year old male who came in complaining about chronic rectal bleeding. It's a common case for this age group and males.
In small biopsy specimens, what we get are small bite fragments from endoscopy exams. Sometimes it's a hit or miss when it comes to sampling like a lot of microscopic examinations are really dependent on how good the clinician was able to sample the tumor suspected to arrive at the correct diagnosis.
Sometimes we get granulation tissue from the colon which is something like a healing edge of an ulcer but not the actual tumor so it ends up not being diagnostic at all.
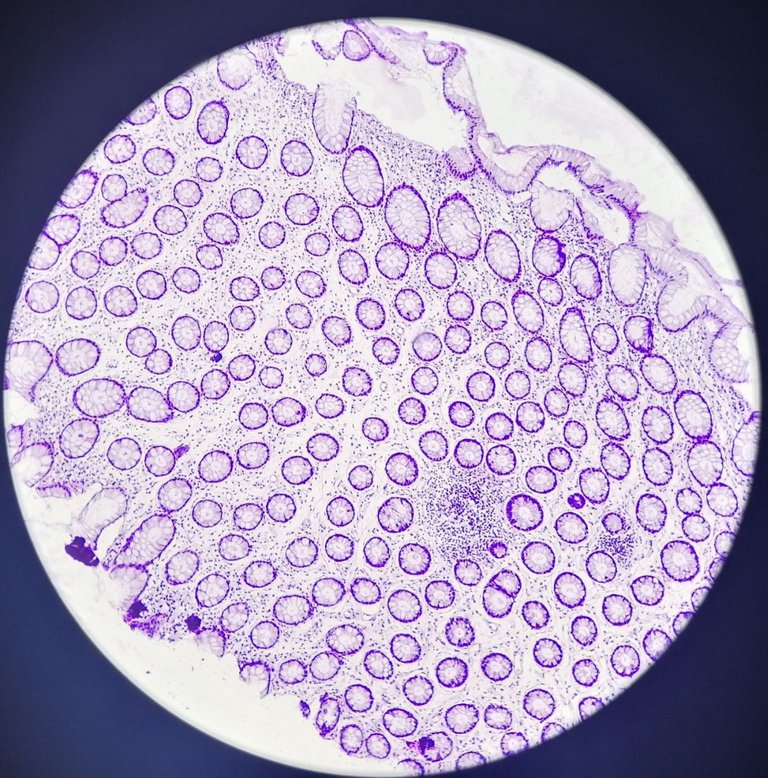
This is at 100x magnification of what a normal arrange of the colonic mucosa would look like at cross section. You'll see glands lined by simple columnar epithelium. Though this angle doesn't reveal a lot about the stroma but it's generally benign looking.
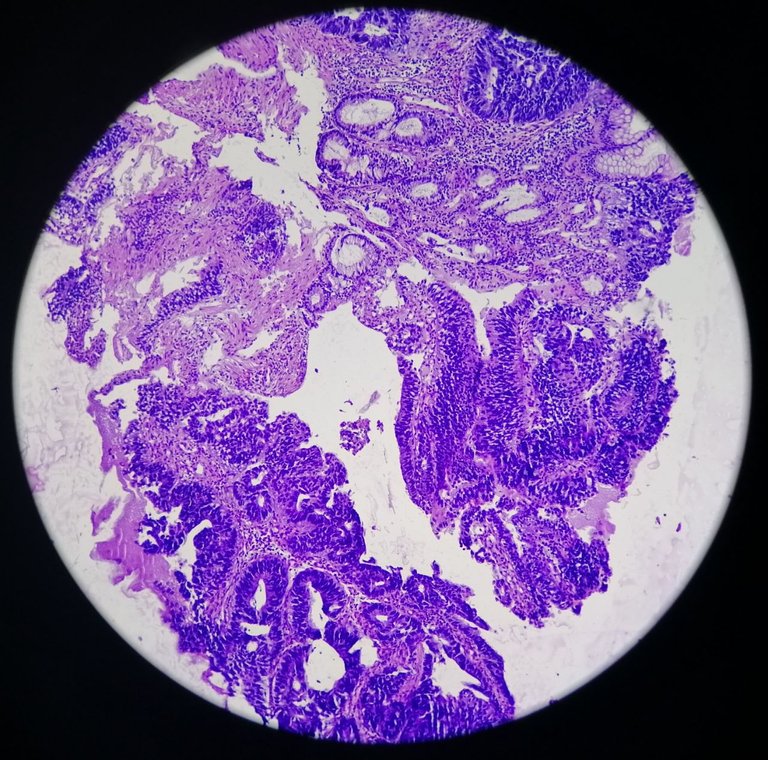
Taken at 100x magnification, taken from the same sample, you'll immediately appreciate how the abrupt change in architecture hints malignancy.
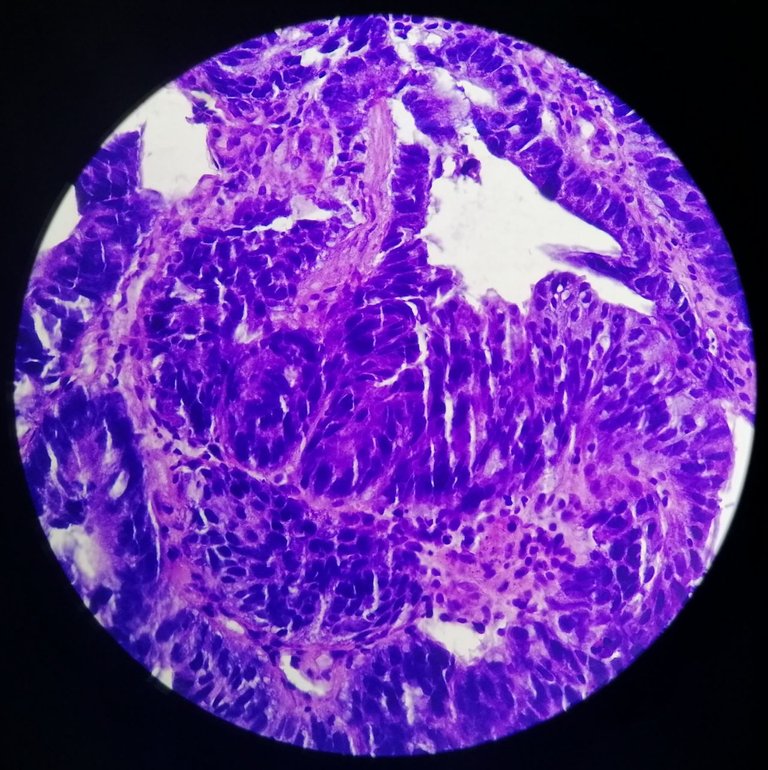
Taken at 400x magnification, you'll see the loss of order in the glands and it's invading the stroma supporting the mucosa. The cells would have a hyperchromatic (more blue), round to pleomorphic nuclei with inconspicuous to prominent nucleoli and moderate to abundant cytoplasm.
Grading this depends on the architecture, back then the terms well-differentiated, moderately differentiated and poorly differentiated were used. Now we can label it as low grade vs high grade where low grade (well to moderately differentiated) and high grade (poorly differentiated) is the tagging.
If you can appreciate the tumor with well formed glands, then it's well differentiated. If there is some cribriforming or slight solid patterns showing, then it can be moderately differentiated. The poorly differentiated tagging is used when you can't appreciate the tumor as a gland and it's predominantly composed of solid sheets to single infiltrating cells.
The prognosis is correlated with the forms they look with poorly differentiated having the worse. But it also depends on the stromal invasion and lymph node spread.
This is just a TL:DR version of how to describe the tumors we see. There's a lot of reading to do when it comes to classifying it based on morphology and correlating the specimen with the clinical history but those are stuff you won't find practical use knowing right now.
My approach to blogging about my work is focused on the nice to know trivia approach and trying not to bore people with too much info.
If you made it this far reading, thank you for your time.
Posted with STEMGeeks
!1UP
You have received a 1UP from @luizeba!
@stem-curatorAnd they will bring !PIZZA 🍕
Learn more about our delegation service to earn daily rewards. Join the family on Discord.
I like the patterns in the first picture