The mechanism of Child Birth | Normal Labour
Hey guys, welcome to my new article. In my previous article, I discussed the basics of reading an abnormal chest X-ray. In this article, we will discuss how normal labour occurs and what are the factors affecting normal labour. Labour is the series of events that happen in the genital organs to expel the baby out of the womb. If this starts before the 37 completed weeks, it's known as preterm labour. Also, we must know the difference between labour and delivery. Delivery means the expulsion or extraction of the baby out of the womb. See, delivery can take place without labour as in the Cesarian section. Therefore, the delivery may be vaginal or abdominal.

Credits, Needpix, Reuse license
Normal Labour (Eutocia)
A pregnant woman is said to have normal labour if only these requirements are met. The labour must be at term, which means it should be after 37 completed weeks and before 42 weeks. The baby should have a vertex presentation, meaning the head must be the part to come out first. There must be no unwanted prolongation of the labour. There must be a natural termination with minimal support and finally, there must be minimal complications.
Any deviation from these criteria leads to abnormal labour. Where the presenting part can be other than the head and various other complications modifying the nature and course of the labour.
A mechanism of normal labour involves the movement of the fetus through the genital organs and the bony pelvis. This process involves the widest diameter of the fetal head and the widest diameter of the maternal pelvis. This makes the traveling route easier for the baby. There are key steps that describe the route that a fetus has to cover to come out of the womb. Here are those key steps.
- Engagement
- Descent of the fetus
- Flexion of the neck
- Internal rotation
- Crowning of the head
- Extension
- Restitution
- External rotation
- Trunk expulsion with lateral flexion
so, before we get into this topic, we need to have a basic idea about the anatomy of a maternal pelvis.
Anatomy of Pelvis
A normal pelvis consists of 4 bones, 2 nominate bones, 1 sacrum, and 1 coccyx united together by 4 joints. The pelvis is mainly classified into the true and false pelvis. False pelvis means the part of the pelvis formed by the iliac bones and is of very little signification during labour. True pelvis is what we need to focus on. True pelvis is of chief concern because it forms the canal through which the fetus passes. True pelvis is further divided into the inlet of the pelvis, cavity, and outlet of the pelvis.
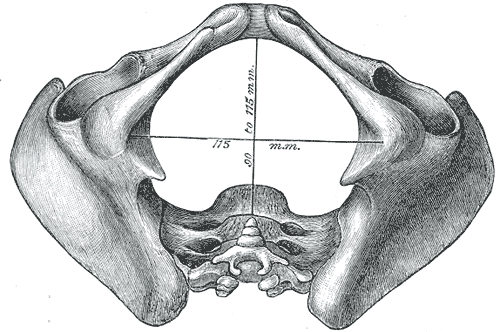
**Inlet of the Pelvis**: This refers to the pelvic brim with the almost round shape, and shortest anterior-posterior diameter. There are various diameters that might affect the course of labour.
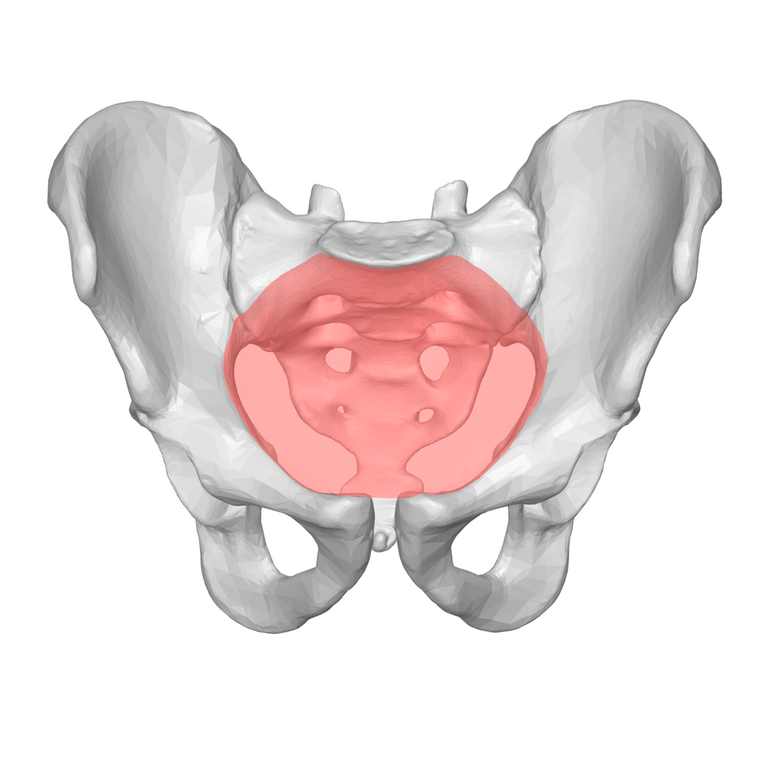
Image: Inlet of Pelvis (Credits, Wikimedia, Resue license)
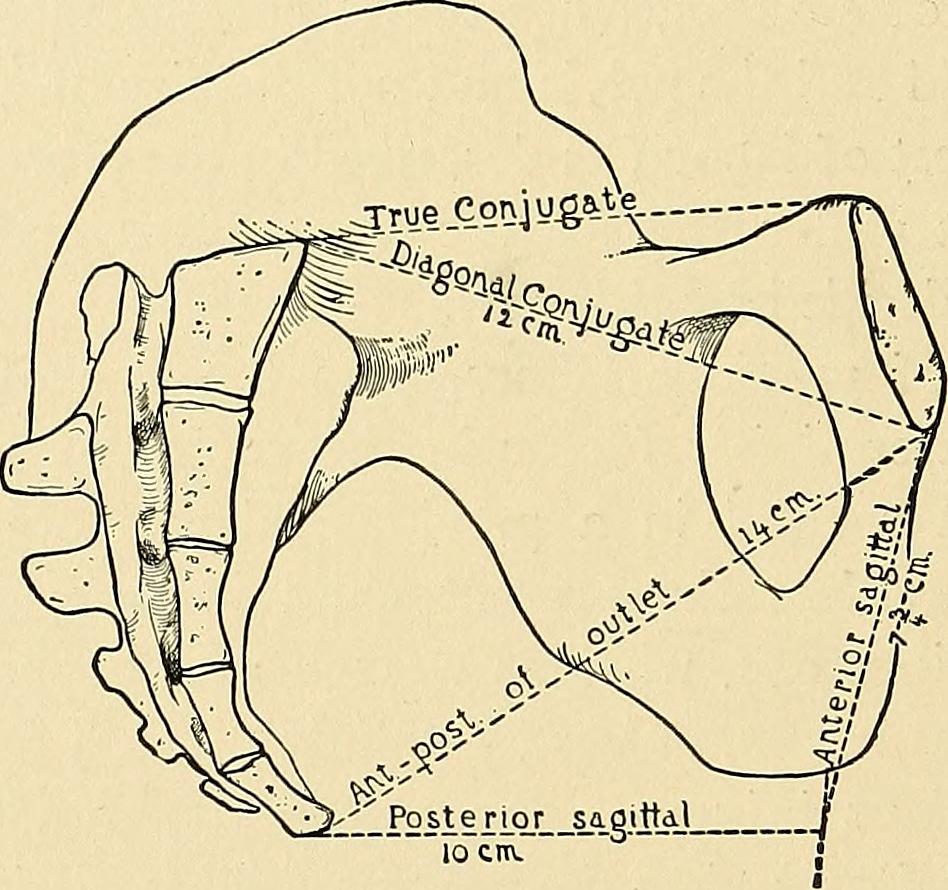
- Ture conjugate: this diameter extends from the midpoint of the sacral promontory to the inner margin of the upper part of symphysis pubis measuring about 11 cm.
- Diagonal conjugate: This diameter extends from the sacral promontory to the lower part of the symphysis pubis measuring about 12 cm.
There are various other diameters but these two the most important once.
The cavity of the pelvis: This part refers to the segment of the pelvis which is bounded above by the pelvic inlet and below by the outlet. The cavity also consists of two diameters and this is also almost round in shape. The diameter of the cavity are as given below.
- Anterior-posterior diameter: Distance between the junction of 2nd and 3rd sacral bones to the midpoint of the symphysis pubis.
- Transverse diameter: Distance between the tissues covering the sacrosiatic notches.
The outlet of the Pelvis: The outlet is the last part of the pelvis and is also almost round in shape in a normal woman. The outlet is formed by these borders. posteriorly, tip of the coccyx, laterally ischial tuberosity, and anteriorly pubic arch. This part also has two important diameters.
- Anterior-posterior diameter: the distance between the tip of the coccyx to the lower part of the symphysis pubis.
- Transverse diameter: the distance between two ischial spines.
This was the basic idea for the anatomy of the pelvis. Now we can move on to the different mechanisms that occur during the labour. The key steps of labour are already mentioned above. Let's start with the Engagement of the head.
Engagement of the Head
This is the first step in the mechanism. Engagement is said to be done when the vertex(head) is at the level of the pelvic inlet. The widest part of the head(biparietal diameter) measuring about 10 cm engages with the maternal pelvis. In normal labour, the head enters the pelvis through the available transverse diameter in about 70% of the cases and lesser through other oblique diameters, Therefore, the position of the head can be described as occipito-transverse position.
The sagittal suture may not correspond directly to the transverse diameter of the of the pelvis. There might be some degree of deflection.
Descent of the head
This means the fetus is descending down to the pelvis. In a primigravida woman(pregnant for the first time), the decent is usually in late stages, but in a multigravida woman(pregnant multiple times), the descent and engagement usually start with the engagement of the head. There are some factors that facilitate the decent:
- Regular uterine concentrations and retractions.
- Bearing down efforts.
- Rupture of the membrane or water broke.
- Increased tone of muscles.
Flexion of the neck

After the engagement and descent of the fetal head into the maternal pelvis, there is huge resistance from the maternal pelvic floor muscles. This causes the flexion of the head into the thorax.
when the pelvis is adequate, the flexion is achieved by the unfolding of the cervix or from the resistance offered by the muscles. Also, this step is very necessary, because this reduces the diameter of the head to which makes it easier to pass through the pelvis
Internal Rotation
During engagement, decent, and flexion of the neck, the head is in a transverse position due to various anatomical reasons. After the complete decent, it reaches the pelvic floor. The pelvic floor has got the shape of the gutter, due to muscles like pubococcygeus and iliococcygeus. This encourages the fetal head to rotate about 90o
Thus, the head rotates from the occipito-transverse position to the occipito-anterior position. It must be noted that it's a slow process, and a little bit of rotation happens with every uterine concentration. It keeps on rotating until it achieves nearly 90 degrees. The factors contributing to the internal rotation of the head are:
- The downward slope of the pelvic floor.
- Forward Inclination of the pelvic walls.
- Unequal flexibility of different parts.
Only the head is rotated, the shoulder remains in the anteroposterior position. This causes the torsion of the neck. This phenomenon is nearly inevitable. The neck cannot sustain this type of pressure, therefore there is some degree of rotation in the shoulder too.
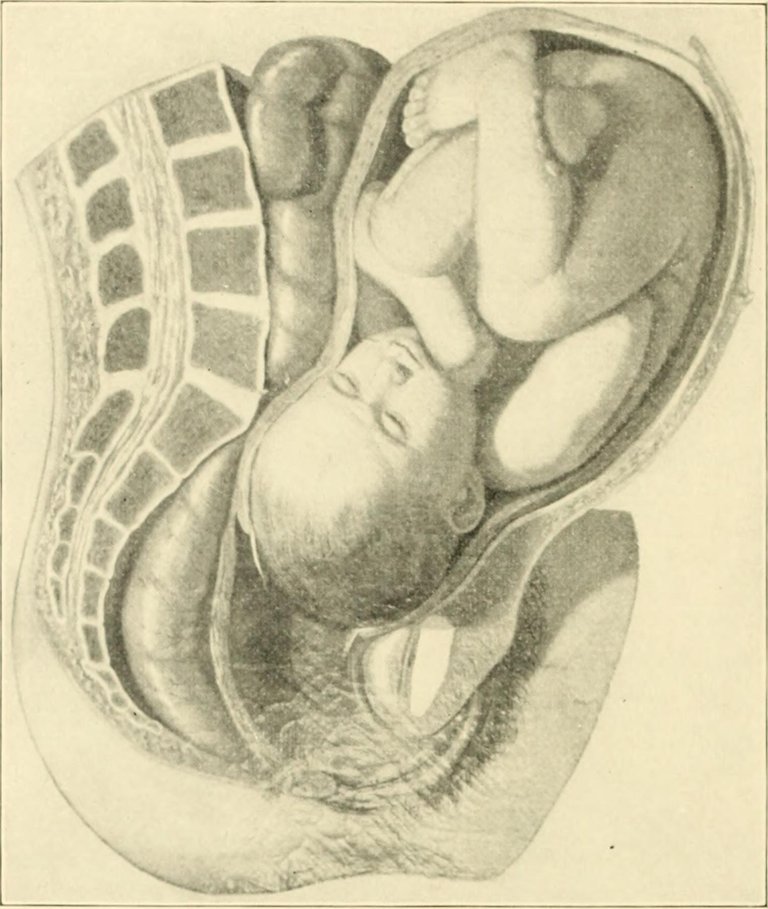
Crowning of the head
Crowing is the stage where the head of the baby starts to appear at the vulva. After the internal rotation of the head, more decent occurs. The maximum diameter of the head which is biparietal diameter starts coming out. This in turn stretches the vulva and does not revert back even after the contraction is over.
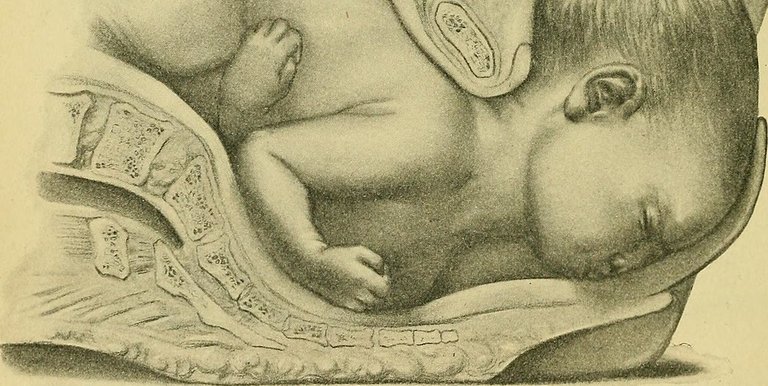
Image: Crowning of the head (Credits, Flickr, Reuse license)
The complete delivery of the head is completed at this stage and the mother is more encouraged.
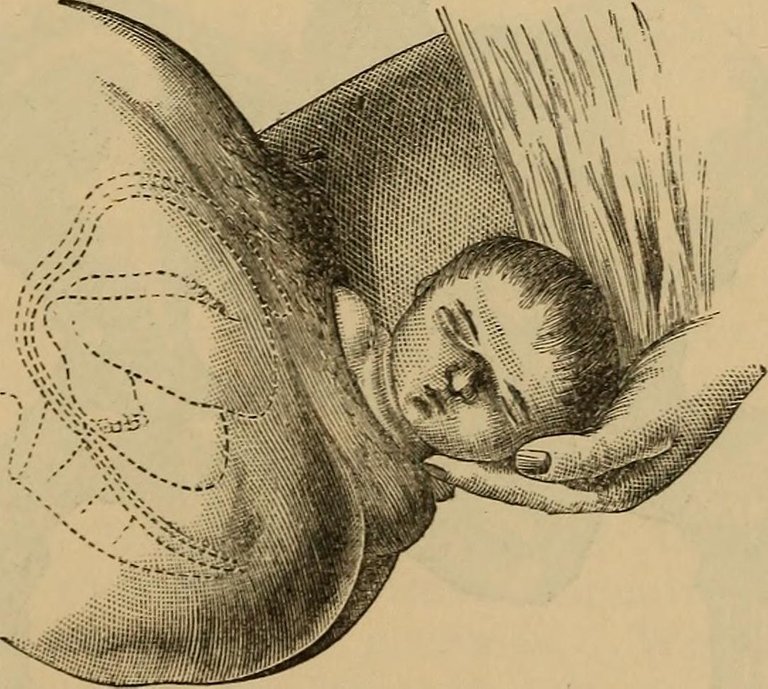
Extension of the head
After the crowing, the head stats coming out and is extended. This means the head is now completely delivered in an extended state. This happens through "Couple of force" theory. The force from the uterine concentrations pushes the head in the downward direction and the resistance from the pelvic floor pushes the head in an upward direction. The presenting parts are vertex, brow, and face. After this, the chin is immediately delivered.
After the delivery of chin, the head drops down, bringing the chin in close proximity to maternal back.
Restitution
As, I said, in internal rotation, torsion of the neck occurs, due to heavy rotation of the neck without the rotation of the shoulder. So, in this step, after the complete delivery of the head, it rotates back to its original position. it means it rotates back 90 degrees. Also, it causes the untwisting of the neck.
The occiput thus points the maternal thighs.
External Rotation
Restitution and external rotation happens at the same time. It's the same as restitution, the moment of rotation of the head is visible by the doctor, due to internal rotation of the shoulder. The anterior shoulder now attains the anteroposterior diameter.
The occiput now directly points toward the thighs of the corresponding sides which was also the original position as in the 1st step(engagement).
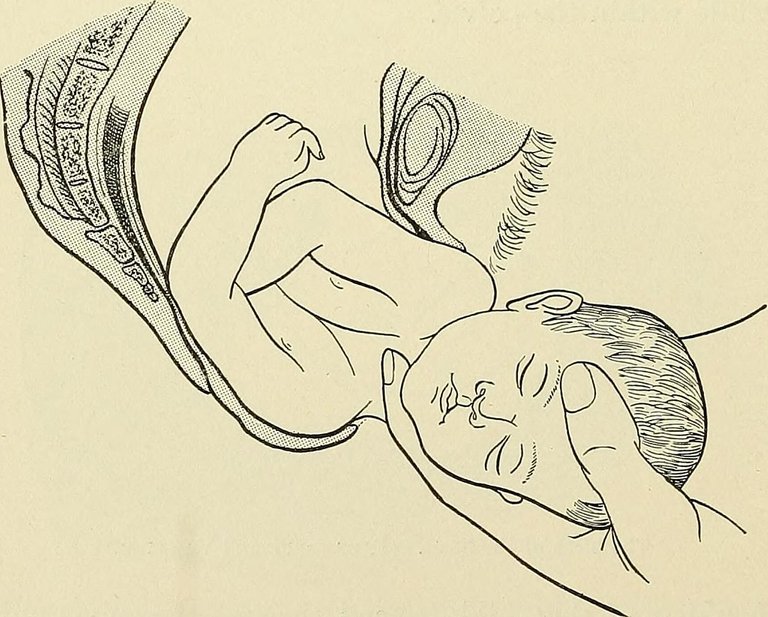
Birth of Shoulder and Trunk
{kind=link}
{kind=link}
_(14797758483).jpg){kind=link}
This is the final step of the mechanism of labor. After the shoulders are in the anteroposterior diameter of the outlet of the pelvis, further descent occurs, this can be natural or might be due to downward traction by the medical staff. This force or pressure causes the escape of the anterior shoulder from the symphysis pubis.
Finally, by providing the upward force and assisting the baby, the posterior shoulder is also delivered and the rest of the trunk is expelled easily.
This is how a child is born.
That's it for this article guys, hope you liked it.
*All images used are copyright free and are provided with appropriate credits*
References:
https://geekymedics.com/mechanism-of-labour/
https://www.uptodate.com/contents/management-of-normal-labor-and-delivery
https://www.glowm.com/section_view/heading/anatomy-of-the-pelvis/item/95
https://www.msdmanuals.com/professional/gynecology-and-obstetrics/normal-labor-and-delivery/management-of-normal-labor
https://brooksidepress.org/Products/Military_OBGYN/Textbook/LaborandDelivery/mechanism_of_normal_labor.htm
Congratulations @idoctor! You have completed the following achievement on the Hive blockchain and have been rewarded with new badge(s) :
You can view your badges on your board And compare to others on the Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPDo not miss the last post from @hivebuzz:
Support the HiveBuzz project. Vote for our proposal!
This is interesting. I was with my wife when she gave birth to our first baby. At what point is the woman told to stop pushing? I'm asking this question because the force with which the baby came out was quite much and it took a bit of expertise from the matron to catch the baby.
it's quite an experience for a mother. I have seen this a few times. It's very painful on their first delivery, so they have a greater urge to Push. we don't tell them to stop pushing till the shoulder of the baby is out. it might take 30 minutes to a few hours, considering the energy mother has left.
Btw, thanks for your question.
Very interesting explanation. Thanks for sharing.
!discovery 30
This post was shared and voted inside the discord by the curators team of discovery-it
Join our community! hive-193212
Discovery-it is also a Witness, vote for us here
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider supporting our funding proposal, approving our witness (@stem.witness) or delegating to the @stemsocial account (for some ROI).
Thanks for using the STEMsocial app and including @stemsocial as a beneficiary, which give you stronger support.