Cardiac Electrophysiology || Extrinsic Cardiac Control
The heart has the ability to conduct both intrinsic and extrinsic. The heart can depolarize itself without the help of the nervous system being an extrinsic innervation of the heart rate although this is done also. The heart actually can depolarize itself, sending action potentials to other parts of the heart such as the myocardium of the heart, and it is known as Automaticity.
In my previous post, I discussed "Cardiac Electrophysiology || Intrinsic Cardiac Condition" and I explained how positive ions get into the SinoAtrial (SA) node cells and the contractile cells thereby creating electricity potentials, which allows the heart to beat by itself. Today, let's touch on extrinsic cardiac conduction of the heart. This has to do with looking at how to increase the heart rate beyond Sinus Rhythm, and how to decrease the heart rate below the sinus rhythm.
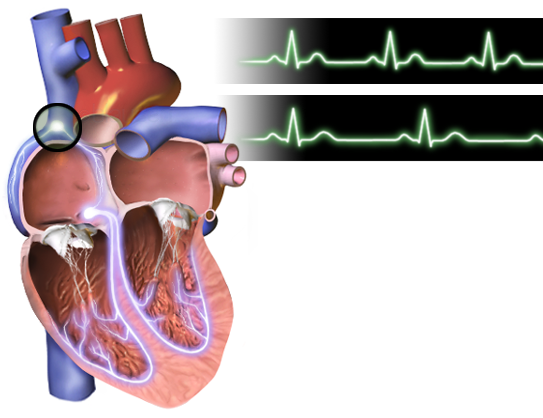
In the SinoAtrial (SA) node cells, the sympathetic nerve releases norepinephrine and epinephrine the beta-1 adrenergic receptor activating intracellular processes such as G-stimulatory protein which gets rid of GDP and binds GTP which turns the stimulatory protein on. The stimulatory protein activates the effector enzyme known as Adenylate cyclase which is responsible for converting ATP into Cyclic AMP which can activate protein kinase A. Protein Kinase A targets L-type calcium channels and phosphorylate them causing the channels to open allowing calcium to get into the cell. When calcium gets into the cell, it depolarizes the cell causing action potentials which increase the heart rate. This can lead to tachycardia such as during exercise.
If the opposite is to be achieved, the parasympathetic neurons would be activated releasing acetylcholine from the vagus nerve. Acetylcholine binds to the muscarinic type 2 (M2) receptor to activate G inhibitory protein which includes alpha inhibitory, beta inhibitory, and gamma inhibitory. The binding causes the alpha to separate from the beta and the gamma inhibitory. The Beta and Gamma inhibitory subunit binds to the membrane channels allowing potassium movement out of the cell, allowing the cell to lose positive ion from the cell causing it to become more negative and decreasing the depolarization rate, leading to a decrease in heartrate below sinus rhythm, and decrease in action potential thereby hyperpolarizing the cell leading to bradycardia. The alpha inhibitory unit inhibits the adenylase cyclase preventing ATP conversion to Cyclic AMP which causes a drop in cyclic amp levels, calcium level, and the heart rate.
In the Contractile cells, the sympathetic neurons allows protein kinase A level to increase, which then phosphorelates the phospholamban stimulating the the membrane and geting in lots of ions into the sarcoplasmic reticulum. The protein kinase A also add phosphate into the voltage gated calcium channel allowing more calcium into the cell stimulating ryanodine type 2 receptors, leading to a lot of calcium in the sarcoplasm which leads to more interaction with the troponin which moves the tropomyosin causing an increased cross bridge formation which would increase the power stroke, ans sliding of the myofilaments which would increase the contraction which would increase the pumping of the heart, the stroke volume, cardiac output and also blood pressure.,
{kind=link}
Thanks for your contribution to the STEMsocial community. Feel free to join us on discord to get to know the rest of us!
Please consider delegating to the @stemsocial account (85% of the curation rewards are returned).
Thanks for including @stemsocial as a beneficiary, which gives you stronger support.